
AuDHD and Pathological Demand Avoidance (PDA)
For Adults and Parents

I’ve always wondered if, as a person wit AuDHD, do I suffer from PDA, otherwise known as pathological demand avoidance. I also hear from parents who struggle with their children displaying PDA symptoms; so I decided to dig into a little research, create some reflection journal prompts, and give some actionable tips and strategies for adults who feel this way and for parents and teachers to accommodate your child or yourself, instead of activating the amygdala.
Gentle Disclaimer 💜
I’m not a doctor, therapist, or licensed mental health professional.
I’m a late-diagnosed, Neurodivergent human and early childhood educator with a deep special interest in research, learning, and teaching about ADHD, Autism, and mental health.
Everything I share here is for education, reflection, and support—not medical, psychological, or legal advice.
Please:
Use this blog as a starting point, not a diagnosis.
Talk to a qualified professional (doctor, therapist, psychologist, etc.) before making changes to medication, treatment, or major life decisions related to your health.
Remember that your brain, body, and story are unique—what resonates for me or others may not be the exact fit for you, and that’s okay.
If you’re ever in crisis or worried about your safety or someone else’s, please reach out to local emergency services or a crisis hotline right away. You deserve real-time, real-world support—not just words on a screen. 💫
Now, on to the Topic:
AuDHD and Pathological Demand Avoidance: A Guide for Neurodivergent Adults, Parents, and Teachers
Introduction
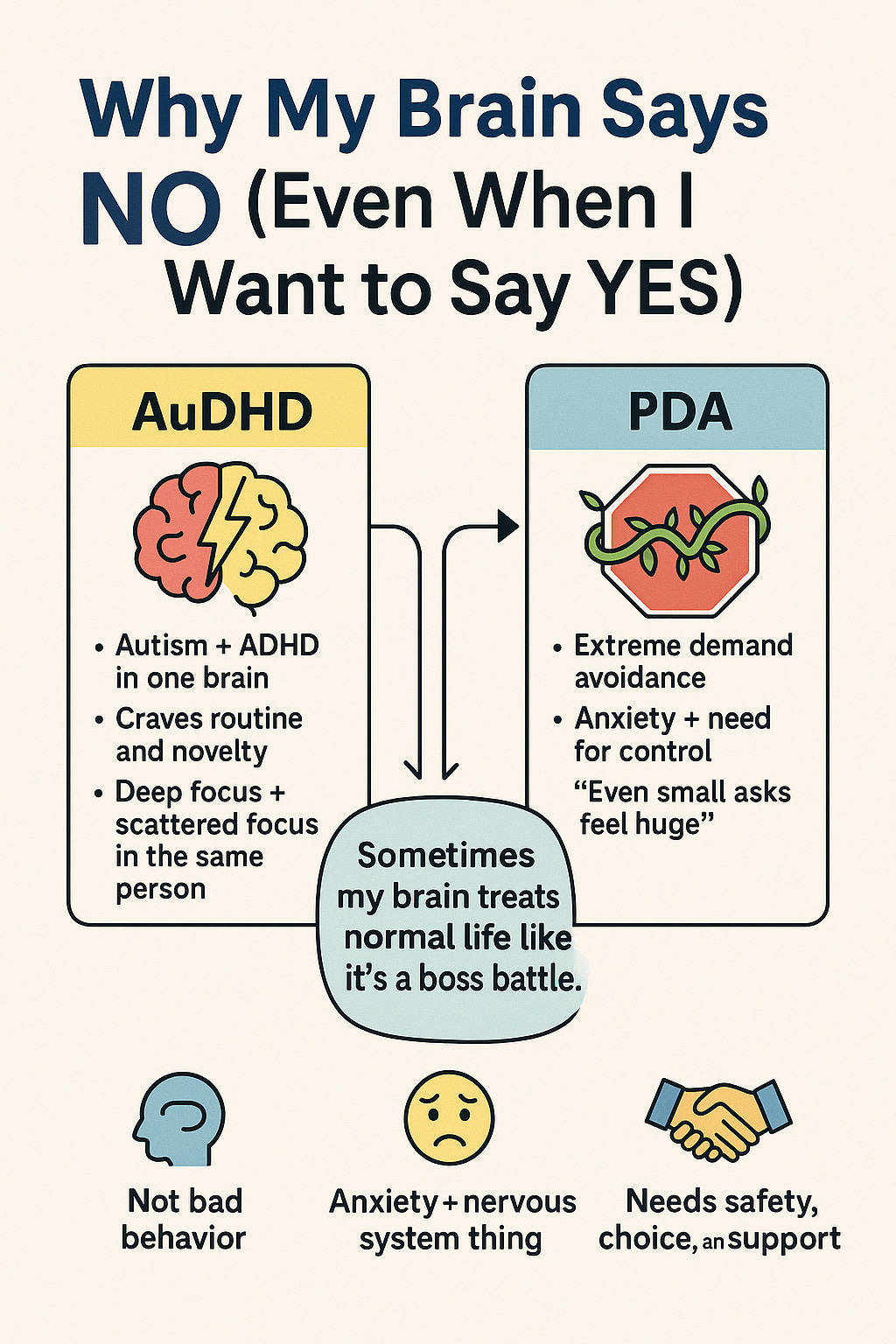
Imagine your brain hitting the “stop” button the moment someone tells you to do something – even if it’s something you actually want to do. Or picture feeling like you’re driving with one foot on the gas and one on the brake at the same time. If these scenarios sound familiar, you might relate to two concepts gaining attention in the neurodivergent community: AuDHD and Pathological Demand Avoidance (PDA).
AuDHD isn’t a typo – it’s a mash-up of autism and ADHD, reflecting a person who is both autistic and has attention-deficit/hyperactivity disorder. PDA, on the other hand, describes a profile (often associated with autism) where an individual fiercely avoids everyday demands and expectations, driven by anxiety and a need for control.
This blog post will break down what each of these terms means and why they occur from a neuroscience and practical perspective. Whether you’re a neurodivergent adult juggling autistic and ADHD traits, or a parent/teacher supporting a neurodivergent child, we’ll explore how these phenomena show up in both kids and adults. We’ll also share some strategies for coping and supporting each other, and end with reflection journal prompts to help you delve deeper into understanding yourself or your child/student. Let’s dive in with a conversational (and occasionally humorous) approach to these serious topics.
What is AuDHD?
AuDHD (pronounced “awed-HD” by some) is an unofficial but popular term that stands for being autistic and ADHD at the same time. In more clinical terms, it means someone meets the criteria for autism spectrum disorder (ASD) and attention-deficit/hyperactivity disorder. Both ASD and ADHD are neurodevelopmental conditions – they affect how the brain develops and works, influencing things like attention, behavior, and social interaction.
Not long ago, it was commonly believed that a person couldn’t have both autism and ADHD. In fact, before 2013 the diagnostic rules (in the DSM-IV) did not permit an ADHD diagnosis for an autistic person. This changed with the DSM-5, and we’ve since learned that autism and ADHD not only can co-occur, but they do so quite often.
Research estimates vary, but studies have found a significant overlap. For example, about one-third of children with ADHD also have autism, and roughly one in ten children with autism have ADHD. Other research suggests the overlap might be even higher – one review found around 40% of those with ADHD meet criteria for autism (and vice versa), and if you include milder traits, the overlap could be up to 80%. In short, AuDHD is more common than you might think.
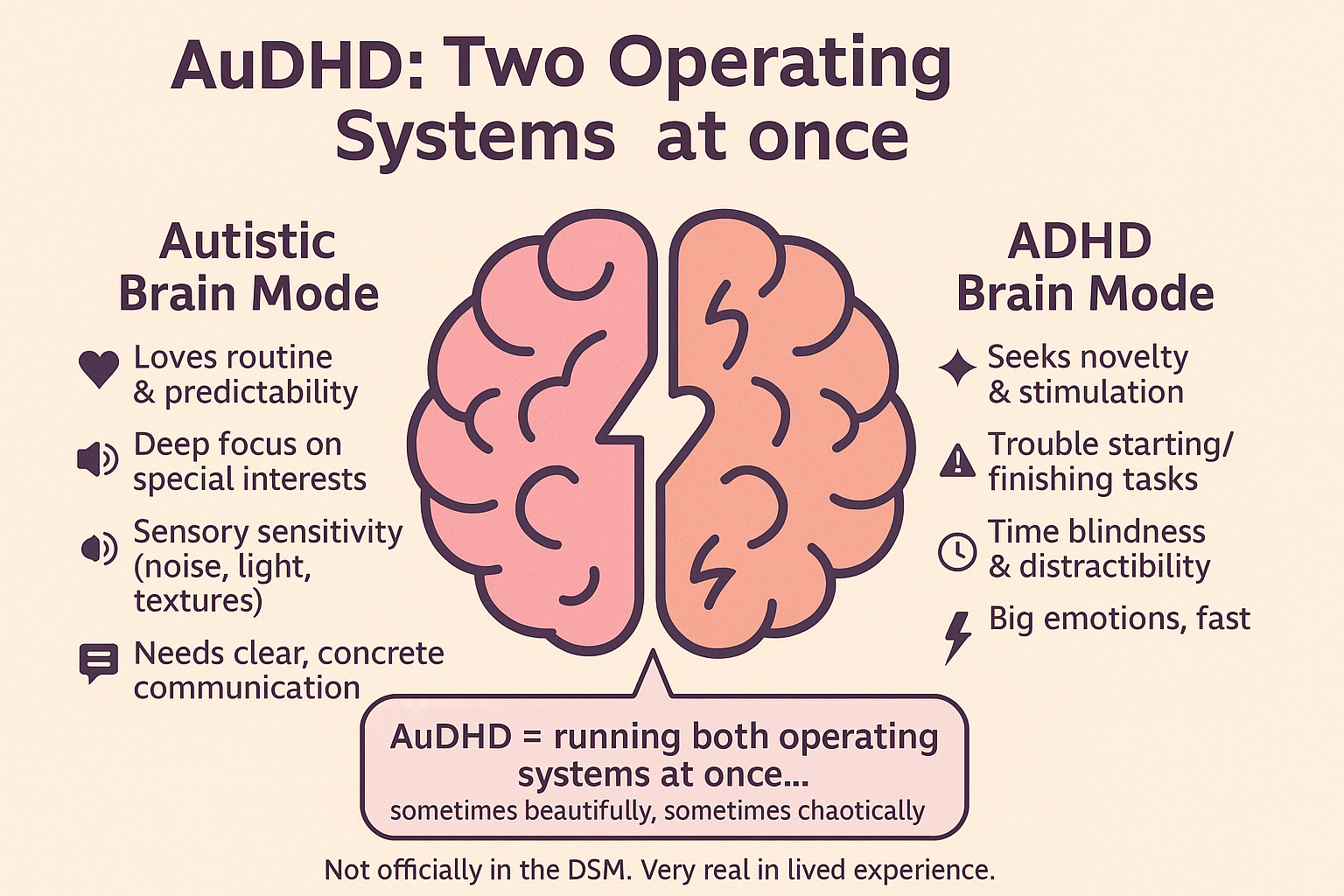
Why have both conditions at once? Part of the reason is that autism and ADHD share some similarities. Both affect the brain’s executive functions (skills like planning, impulse control, and working memory) and can make social communication challenging. At the same time, they also have almost opposite tendencies in other ways. Autistic individuals often love routine and predictability, while ADHD brains seek novelty and stimulation. A person with autism might focus intensely on one task at a time, whereas someone with ADHD might juggle five things at once. You can imagine that having both leads to a bit of an internal tug-of-war.
“I often feel like a living contradiction. I want order but cannot maintain it... I want to be systematic and precise but struggle with it, which leaves me constantly feeling not good enough,” — an adult with AuDHD describing the push-and-pull between autistic and ADHD traitspsychiatry.org.
This quote captures the essence of AuDHD: the conflict and contrast between two neurodivergent profiles. For instance, an AuDHD person might crave structure and consistency (an autistic trait) yet feel painfully bored or restless with the same routine after a while (an ADHD trait). They might get easily overwhelmed by sensory input like an autistic person, but also constantly seek stimulation and new interests like someone with ADHD – a recipe for exhaustion if not managed well.
The term “AuDHD” itself isn’t a formal medical label – you won’t find it on an official diagnosis report. It’s a community-coined term adopted by many neurodivergent individuals to describe their dual identity. Using this label can be validating; it acknowledges that the person isn’t just “autistic with a side of distractibility” or “ADHD but kinda socially awkward” – they fully embody both neurotypes. Recognizing this combination is important because it can affect how someone should be supported. For example, traditional ADHD strategies (like stimulant medications or reward systems) might not fully work for an AuDHD person if their autistic side also needs consistency or sensory accommodations. Likewise, supports for autism (such as clear routines or social skills training) might need tweaks to account for ADHD-related impulsivity or attention issues.
Research into AuDHD is still emerging, but it’s clear that individuals with this dual diagnosis often face extra challenges – and also possess unique strengths. Studies have noted that children with combined ASD/ADHD diagnoses experience higher levels of anxiety, depression, and daily functioning difficulties than kids with either condition alone. It’s as if the challenges can compound. On the flip side, many AuDHD adults and kids develop incredible creativity and problem-solving skills, using one set of traits to compensate for the other. For instance, an AuDHD student might channel their ADHD energy and hyperfocus into a special interest, excelling in that area, or use autistic attention to detail plus ADHD spontaneity to come up with innovative ideas. Every AuDHD person is different, but embracing both parts of their neurodivergent brain can help them understand why they experience the world the way they do and find strategies that honor their whole self.
What is Pathological Demand Avoidance (PDA)?
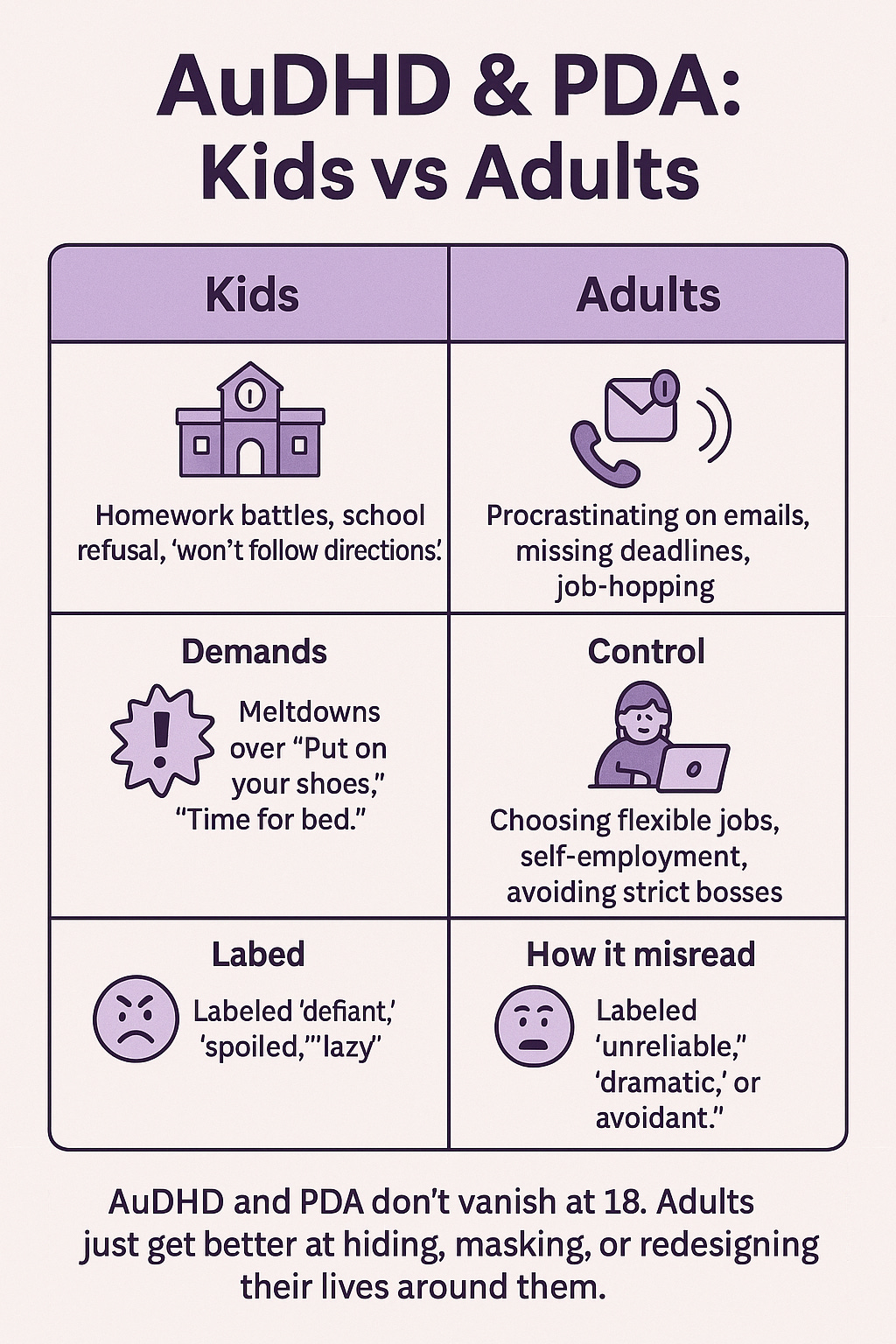
Now let’s talk about Pathological Demand Avoidance, often just called PDA. Despite the intense name, it’s not an official disorder in most diagnostic manuals – rather, PDA describes a behavioral profile seen in some neurodivergent people (most commonly those on the autism spectrum). Essentially, PDA is when a person has a drive to avoid or resist ordinary demands to an extreme degree. We’re not talking about the occasional “I don’t feel like it” attitude; we mean a pervasive pattern where even simple, everyday requests can trigger anxiety and outright refusal. The child who melts down at being told “please put on your shoes,” or the adult who feels a surge of panic when they have to answer an email – that’s PDA in action.
People with PDA aren’t avoiding demands just to be defiant or difficult. In fact, on the surface their behavior might look like defiance or even Oppositional Defiant Disorder (ODD), but the underlying reason is different. Anxiety is usually the key driver. Individuals with PDA experience an intense, internal feeling of discomfort or threat whenever someone else imposes an expectation on them It’s as if an alarm bell goes off in the brain: “Danger – someone is trying to control you!” To extinguish that anxiety, the person avoids the demand by any means necessary. This could mean outright refusal (“Nope, not doing it!”), distraction (changing the subject or making a joke), giving excuses, negotiating to delay it, or in some cases, having a meltdown or running away to escape the pressure
The term “pathological” in PDA is controversial – nobody likes being labeled “pathological,” and it can sound like blaming the person. The intent, however, is to indicate that the avoidance is extreme and clinically significant, to the point that it interferes with daily life. Some advocates prefer to drop the word and instead emphasize the underlying motive. You might hear PDA reframed as “Pervasive Drive for Autonomy” or “Persistent Demand for Autonomy,” highlighting that the person isn’t just avoiding things for no reason – they are driven to maintain their independence and emotional comfort. In fact, PDA was first identified in the 1980s by UK researcher Elizabeth Newson, who described it as a distinct profile of autism where individuals demonstrate a significant need for control to manage anxiety. The profile isn’t officially listed in the DSM-5, but many clinicians (especially in the UK) accept PDA as a helpful descriptor within the autism spectrum.
What does PDA look like day-to-day? A young child with a PDA profile might resist even basic tasks like getting dressed, eating, or playing a game if it’s presented as something they “have to” do. They often insist on doing things on their own terms. For example, they may happily draw a picture when they decide to, but if a teacher says “Please draw this now,” the same activity suddenly provokes distress or refusal. Older kids or teens with PDA might appear oppositional about schoolwork or chores they are actually capable of doing – they might procrastinate until the last minute or only complete tasks when they feel in control. Adults with PDA (yes, they exist – more on that soon) can struggle with typical work and life demands. They often devise creative workarounds to life’s requirements, like choosing jobs that allow a lot of independence, or using technology to automate things (bill paying, scheduling) so they don’t feel the “demand” of doing those tasks manually.
It bears repeating: PDA is not simply bratty behavior or laziness. It’s a serious anxiety-based condition. One clinician explains that for someone with PDA, even a small routine request can feel as daunting as “asking them to climb a mountain,” triggering a fight-or-flight response. Standard discipline or reward tactics tend to backfire, because the more you push, the more the person feels their autonomy slipping away – which raises their anxiety instead of reducing it. Instead, approaches that reduce the sense of demand, offer choices, and emphasize collaboration work best (we’ll delve into strategies soon).
Why Do These Happen? (The Science and Reasons)
Why Does AuDHD Occur?
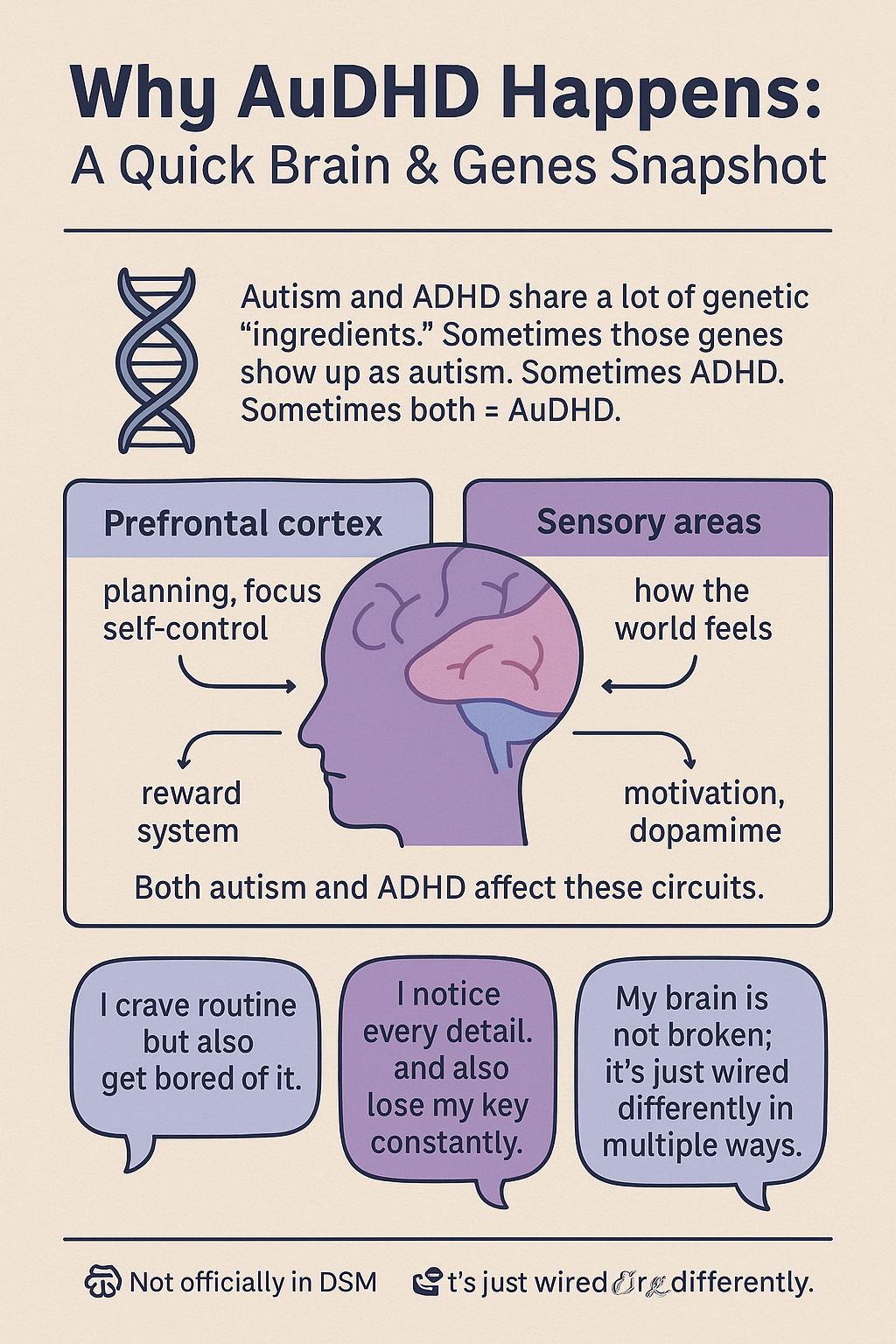
Given how frequently autism and ADHD co-occur, scientists have been investigating the why. One big reason lies in our genes and brains. Autism and ADHD, while distinct conditions, share a lot of genetic underpinnings – in fact, twin and family studies have found roughly a 50% to 70% overlap in genetic factors between the two. Think of it like two different recipes that use many of the same ingredients. If a child inherits a certain mix of genes that affect brain development, those genes might manifest as autism, ADHD, or both. This helps explain why you often see multiple neurodivergent traits in one person or within the same family.
On the brain level, both autism and ADHD involve differences in how the brain’s networks are wired and how brain chemistry operates, especially in regions responsible for attention, impulse control, and reward processing. For example, the prefrontal cortex – the brain’s command center for planning and focus – often shows atypical activity in both autistic and ADHD individuals. If someone’s prefrontal cortex develops in a way that makes focusing and self-regulation hard (an ADHD hallmark) and processes social or sensory information differently (an autism hallmark), that person will likely show signs of both conditions.
Another factor is that autism and ADHD each encompass a wide range of traits. Autism isn’t just one thing – it’s a spectrum – and ADHD symptoms can vary a lot, too. In some individuals, their autism might include traits like inattention or impulsivity that resemble ADHD, and vice versa. Historically, because clinicians weren’t looking for a second diagnosis, these overlapping traits were often missed or misattributed. Now that dual diagnosis is allowed, these “hidden” traits are being acknowledged – for instance, a person can meet full criteria for both disorders, or they might have one diagnosis plus subclinical traits of the other. In other words, someone may not tick every box for an autism diagnosis but still have many autistic-like traits alongside their ADHD (or vice versa). The concept of AuDHD encourages a more nuanced view of neurodivergence that isn’t siloed into single labels.
From a developmental standpoint, having both autism and ADHD can sometimes create a self-reinforcing cycle. For example, imagine a child with ADHD who is super active and struggles to sit still – if they’re also autistic, they might not pick up on the subtle social cues (like a teacher’s impatient expression) that other kids use to realize “Oops, I should calm down.” So the hyperactivity might be even harder to rein in, which could lead to more negative feedback and anxiety. Conversely, an autistic child who intensely focuses on a narrow interest might seem inattentive to everything else, thus appearing to have ADHD (and in fact meeting criteria for it). The two conditions can intertwine in complex ways within one person.
The upshot: AuDHD occurs largely because autism and ADHD have common roots in the brain and genetics, and being wired a certain way can affect multiple aspects of neurodevelopment. Recognizing this overlap helps in practice – it tells us that an AuDHD brain might need support in multiple areas at once. The person isn’t “too complicated” or “weird” for having dual traits; it’s actually an expected outcome of how their brain is built. Importantly, understanding this overlap reinforces that neither autism nor ADHD is caused by “bad parenting” or personal failures – they are part of someone’s neurological makeup from early on.
Why Does PDA Happen?
PDA is a newer concept on the research front, but experts have some theories as to why certain people develop this extreme demand-avoidant profile. At its core, PDA seems to be an anxiety-driven mechanism. One explanation links PDA to traits common in autism, particularly an intolerance of uncertainty and a strong need for predictability. Many autistic individuals feel distress when they don’t know what’s going to happen next or when their routine is disrupted. For someone with a PDA profile, a direct demand can represent that dreaded unpredictability (“Why do I have to do this now? What will happen if I don’t?”) and thus trigger acute anxiety. Indeed, some research (albeit limited) has found a relationship between PDA behavior and high levels of anxiety and intolerance of uncertainty – essentially, the person needs to know or control what’s coming in order to feel calm. The demand throws their sense of control out of balance, so avoiding the demand is a way to restore equilibrium and relieve that anxiety.
Another factor is the need for control itself.
Avoiding demands is a way for a person to exert control over their environment and protect themselves. Some autistic people manage anxiety by trying to control as many variables around them as possible (for example, sticking strictly to their own chosen routines). If you combine that with a strong will or impulsivity, you get someone who almost reflexively says “no” to anything that isn’t their idea.
It’s not a conscious, thought-out rebellion; it’s more like an instinctive defensive reaction. In psychological terms, you might call it a form of the fight, flight, or freeze response – except the “fight” here can be verbal refusal, and the “flight” might be something like mentally checking out or physically escaping when asked to do something.
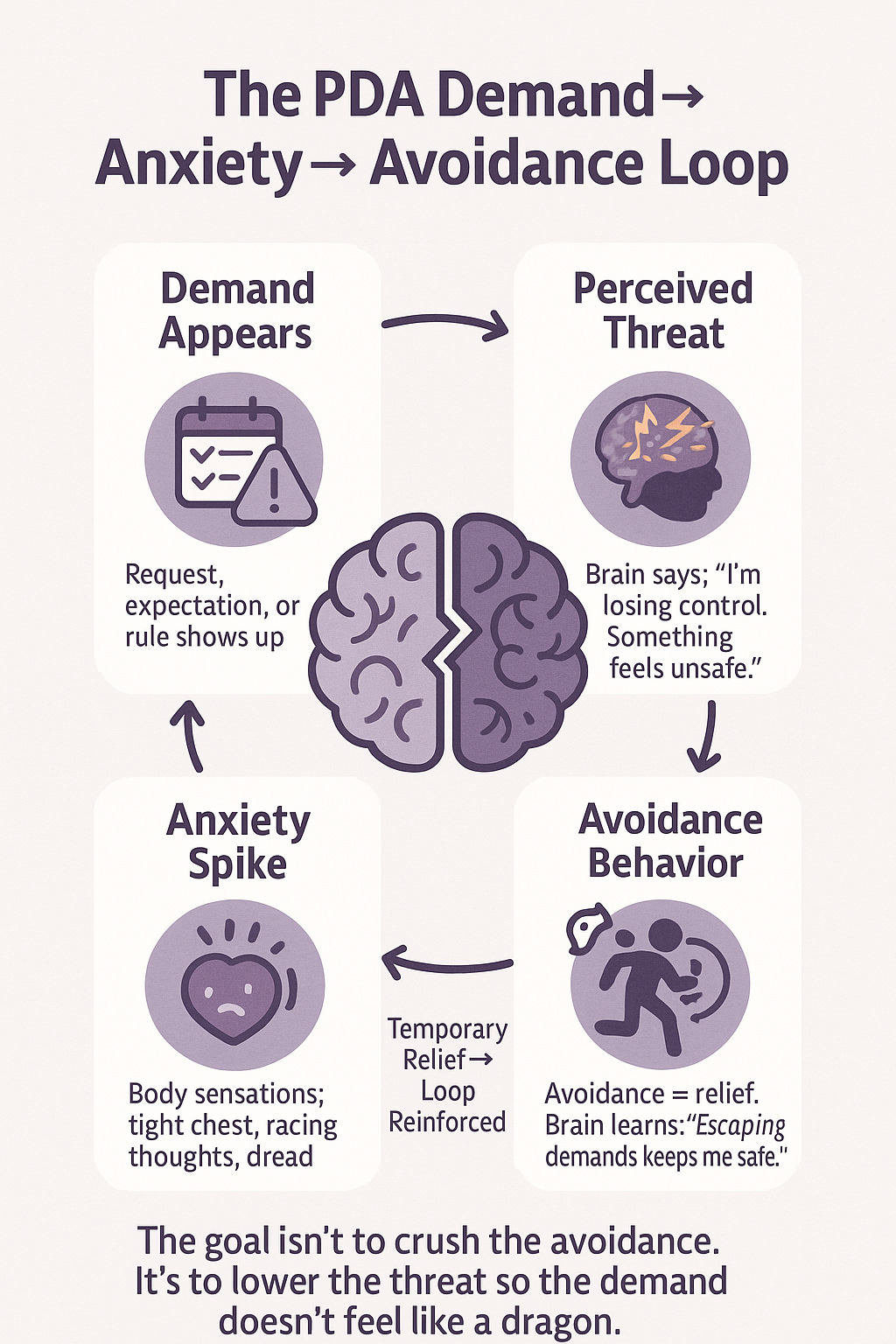
Over time, if a child with this tendency repeatedly finds that refusing gets them out of anxiety-inducing demands, the behavior gets reinforced. They learn “when I say no or freak out, people back off.” Each time they manage to escape a demand and feel relief, it reinforces the avoidance pattern. This is how a coping mechanism can become deeply ingrained.
One thing experts agree on: PDA is not the result of someone simply being spoiled or never disciplined. There’s likely a neurological basis involving how their stress response system works. The brain’s amygdala (fear center) and related circuits may go into overdrive when confronted with demands, even minor ones. In other words, the PDA person’s brain might perceive a request like “Do your homework now” in a similar way that most people would perceive a bear charging at them – it’s sensed as an immediate threat, hence the extreme panic or avoidance. So, punishing a child for this reaction is as futile as punishing someone for flinching at a loud noise; it’s an automatic response, not a deliberate choice.
It’s important to note that research on PDA is ongoing, and the concept has been somewhat controversial. Some clinicians argue that what we call PDA might just be a combination of autism traits and anxiety, or autism plus a touch of ODD. There’s also discussion about whether trauma or environment might play a role for some individuals (for example, did frequent overwhelming demands in early childhood sensitize them to develop PDA?). As of now, PDA is not officially a diagnosis in manuals like the DSM or ICD, and more studies are needed to fully understand it. However, the pattern of extreme demand avoidance is very real to those experiencing it, and many families and professionals find the PDA framework useful for figuring out effective support strategies. In summary, PDA likely happens due to a mix of an autistic processing style, high anxiety levels, and learned patterns of avoiding loss of control. Understanding the “why” behind it helps us respond with empathy and creativity rather than frustration.
Kids vs. Adults: Do These Conditions Only Affect Children?
Short answer: No – both AuDHD and PDA affect adults as well as children. They may first become noticeable in childhood, but they are neurodevelopmental differences that persist throughout life (even if the way they show up can change over time).
AuDHD in adults: Autism and ADHD don’t magically disappear when someone turns 18. Many adults out there are Autistic ADHDers, whether they know it or not. In fact, because the dual diagnosis wasn’t commonly given until recent years, a lot of today’s AuDHD adults weren’t identified as kids. Some might have been diagnosed with one condition but not the other; others were misdiagnosed with something else entirely (or just seen as “quirky” or “lazy”) despite their struggles. It’s increasingly common for adults – especially women and nonbinary folks, who were often underdiagnosed – to realize in their 20s, 30s, or later that they actually fit the profile of both autism and ADHD. This self-discovery can be empowering, giving context to a lifetime of feeling “out of sync.”
Adults with AuDHD continue to experience the blend of traits we described earlier. They might change jobs frequently or have difficulty with the typical 9-to-5 work environment – an ADHD-like restlessness coupled with autistic sensory sensitivities can make conventional workplaces challenging. Socially, an AuDHD adult may have some autistic social differences (like needing more direct communication or more alone time) and ADHD-related impulsivity in conversations, which is a unique mix to navigate in friendships and relationships. On the positive side, many AuDHD adults leverage their dual neurodivergence as a strength. They might excel in creative fields, technology, research, or any area where hyperfocus, attention to detail, and outside-the-box thinking are assets. They often find that learning about both conditions helps them create a personalized toolbox of supports – maybe they use ADHD-oriented strategies like time-management apps plus autism-oriented supports like sensory breaks and visual schedules, in combination.
It’s worth noting that since AuDHD is still an emerging concept, adult healthcare providers or therapists might not all be familiar with it. An adult seeking support might have to educate their providers on their dual needs. Fortunately, neurodivergent adults have formed online communities and resource groups to share experiences about being AuDHD. Finding others who identify as Autistic-ADHD (through social media, forums, or local groups) can be incredibly validating – there’s comfort in realizing you’re not alone and trading tips on navigating work, relationships, and life with this dual neurotype.
PDA in adults: PDA is most often discussed in the context of children (perhaps because extreme demand avoidance in kids leads to obvious struggles at school and home). However, those kids grow up, and yes, adults can and do have PDA profiles. An adult with PDA might not throw toddler-style tantrums when overwhelmed by demands, but they can still feel that intense anxiety and resistance internally. It might manifest in subtler or more socially acceptable ways, such as:
Chronic procrastination: They may find themselves putting off tasks until the very last moment. If something needs doing, they delay and delay – essentially avoiding the demand until the pressure is so high that it feels like their own decision to do it in a rush. (Sound familiar to any adults pulling all-nighters to meet deadlines?) This pattern often isn’t just “laziness” – it’s anxiety about the demand that causes them to freeze or divert their attention, until external urgency forces action.
Difficulty with authority figures or rigid structures: Many PDA adults report struggling in traditional work environments. They might frequently clash with bosses, ignore directives they find arbitrary, or quit jobs impulsively when they feel micromanaged. They often prefer roles with greater autonomy or self-employment to avoid the feeling of being under someone’s thumb.
“Strategic” self-imposed rules: Some adults cope by setting very particular ways of doing things, effectively controlling how a task is done to feel less at the mercy of it. For example, an adult might only do housework at specific times with specific music playing, and if those conditions aren’t met, the demand of cleaning feels unbearable. It’s like they create their own framework for demands to make it feel self-driven.
Relationship tensions: The need for control can spill into personal relationships. A PDA adult might have an extra hard time with compromises or plans made by others. If friends or partners don’t understand why they’re so sensitive to being told what to do, it can lead to arguments or the PDA adult withdrawing. For instance, if their spouse “nags” about a chore, they might shut down or react angrily not out of spite, but because that demand triggered their anxiety. Communication and understanding are key to avoiding misinterpretation in these situations.
Emerging research on adults with PDA traits is shedding more light. One study that adapted a PDA assessment for adults found that autistic adults with a PDA profile tended to have higher levels of anxiety and lower emotional stability (more mood swings or stress reactivity) than other autistic adults. There’s also evidence that intolerance of uncertainty – that need to know what’s coming – correlates strongly with PDA in adults. This all validates what many adults with PDA will tell you: it’s not that they don’t want to accomplish things or cooperate, it’s that the typical way society expects things to be done clashes with how their brain operates. If they aren’t in the mental driver’s seat, panic sets in and their brain hits the brakes.
Anecdotally, some PDA adults say they’ve learned to “game” themselves to cope. For example, they might turn necessary tasks into personal challenges or into a game to make it feel like it’s on their terms (e.g., “Bet I can shower and get ready in under 7 minutes – go!”). Others choose career paths and lifestyles that naturally grant a lot of independence, reducing the number of external demands. In essence, they structure their world to suit their neurotype.
The bottom line is that PDA is not just a phase for kids – it can be a lifelong profile. However, adults often have more freedom to shape their environment than children do, so a PDA adult might intuitively arrange their life to avoid many triggers (which can make their PDA less visible to outsiders). Still, plenty of adults quietly struggle with demand avoidance, sometimes without a name for it until they stumble upon the term “PDA.” Recognizing it can be a lightbulb moment that leads to greater self-compassion and new coping strategies. It’s never too late to understand why you react the way you do and to find ways to work with (rather than against) your brain’s instincts.
Tips and Strategies for Support
Living with AuDHD or PDA (or supporting someone who does) can be challenging, but there are many strategies that can help. Below, we’ve divided tips for different audiences: first for Neurodivergent adults themselves, and then for parents/teachers of Neurodivergent kids. Many of these ideas are useful for everyone, so feel free to read both sections.
Strategies for Neurodivergent Adults (with AuDHD and/or PDA
)
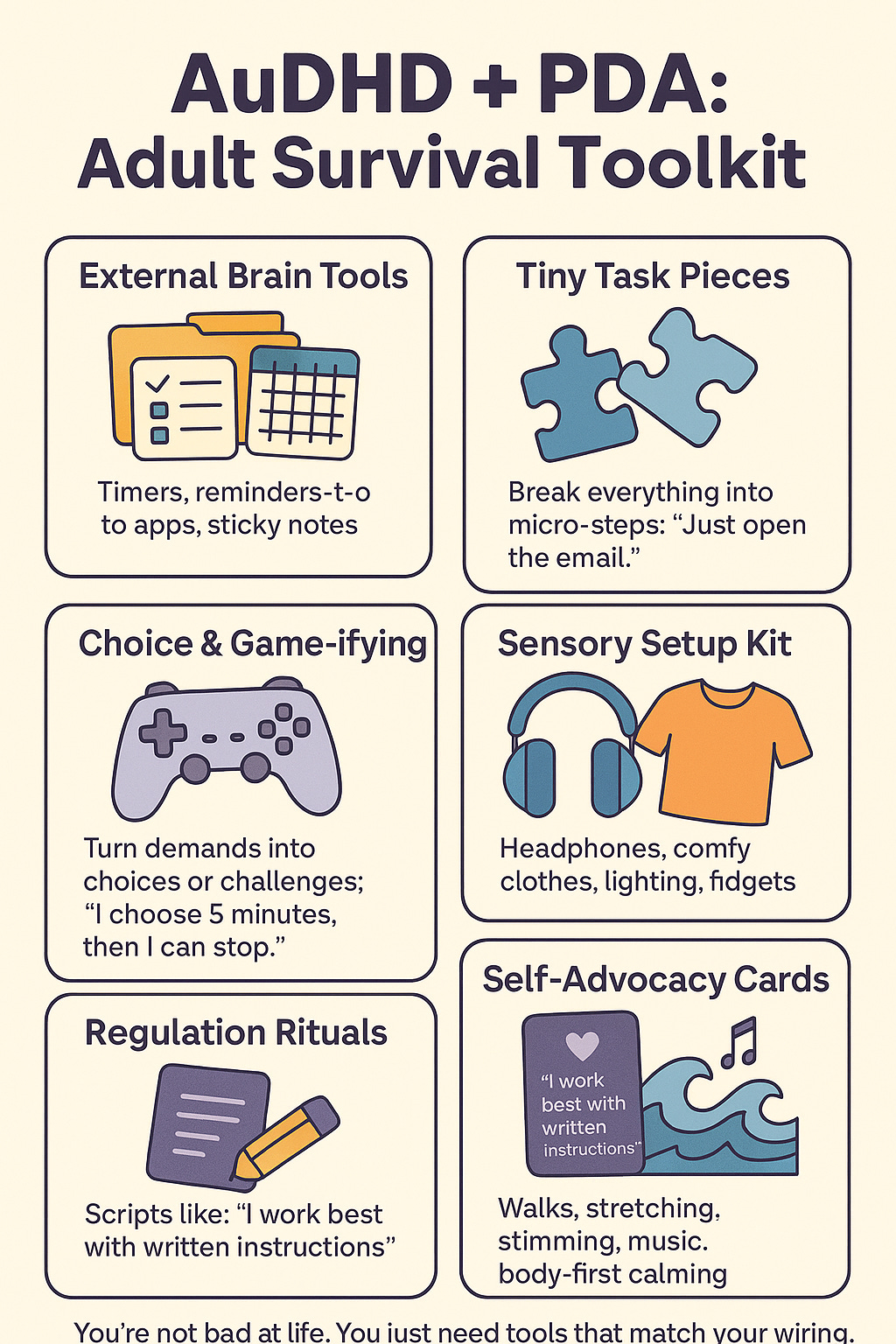
Create structure with flexibility: Finding the right balance of routine and variety is key for an AuDHD brain. Use tools like planners, reminder apps, or calendars to provide gentle structure to your day (helpful for ADHD) while allowing yourself to customize how and when you do things (helpful for autism/PDA). For example, have a morning routine but give yourself the freedom to do the steps in any order, or take breaks in between. This gives a sense of stability without feeling trapped.
Manage sensory and focus needs: Both autistic and ADHD brains can get overwhelmed, though for different reasons – autistic individuals might be over-sensitive to stimuli, while ADHD folks might be under-stimulated and seek input. Set up your environment to support you. This could mean using noise-cancelling headphones in a noisy office, keeping fidget tools at your desk, adjusting lighting at home to be softer, or playing background music/white noise to help concentrate. A well-tuned sensory environment can prevent stress that might otherwise trigger a demand-avoidant meltdown or an ADHD burnout.
Break tasks into bite-sized pieces: If demands tend to paralyze you (PDA-style) or you struggle with starting tasks due to executive dysfunction (ADHD-style), make the task as small as possible. Having to “clean the entire house” is overwhelming; instead, decide to just collect the trash from one room, or just wash five dishes – a tiny, concrete goal. Often, getting started is the hardest part. Once you begin and get a bit of momentum, you might find you can keep going. And if not, that’s okay too – you met your goal, and you can take a break and tackle another small bit later. Little by little gets it done.
Use “choice and control” self-talk: This tip comes from people with PDA: explicitly remind yourself that you choose to do a task and can control aspects of it. If you have to do something unpleasant, try saying (out loud or in your head), “I’m going to do <X> now, because I choose to, and I’ll stop after 10 minutes if I want.” Giving yourself an “out” paradoxically makes it easier to lean in and start. Often, once you begin, you’ll continue longer than 10 minutes – but knowing you have permission to quit can silence that rebellious inner voice. It’s a way of tricking your brain into feeling the task is your decision, not an external demand.
Lean into special interests and strengths: One great thing about neurodivergent minds is that they often come with intense passions or unique talents. Leverage these! If you have AuDHD, you might have the autistic ability to hyperfocus deeply and the ADHD creativity to make connections between ideas. Use that to your advantage. For example, if you love coding and get hyperfocused, structure your work to include coding tasks during your most alert times. Or incorporate your interests into tasks you dislike – if you’re a music lover who dreads exercising, only allow yourself to listen to your favorite album while working out, so the task is paired with something enjoyable. Turning chores or obligations into something personally meaningful or fun can flip them from “demands” into activities you want to do.
Build external executive function supports: Don’t be ashamed to rely on external aids for organization and memory – that’s what they’re there for. Use phone alarms, sticky notes, to-do apps, written schedules, whatever helps get things out of your head and into a reliable system. Many AuDHDers find visual timers or checklists helpful (they provide structure for the ADHD side and clear expectations for the autistic side). Breaking big projects into a series of small checkboxes can give a satisfying sense of progress. These tools act like an “external brain,” helping you stay on track when your internal executive function is zig-zagging.
Practice self-advocacy and communication: You have every right to have your neurodivergent needs accommodated in adult life, too. If you’re comfortable, let the people close to you know about your triggers and preferences. For example, telling a partner, “Last-minute changes really stress me out; I’d appreciate if we could set plans in advance when possible,” can prevent misunderstandings. Or informing your boss, “I work best when I have written instructions and a clear deadline,” can get you what you need to succeed. You can share as much or as little as you’re okay with – even simply saying, “I have trouble with XYZ, so can we try doing ABC?” without delving into diagnoses, is advocating for yourself. The more your environment is shaped to fit you, the less you’ll run into those panic-inducing demand clashes.
Manage stress and plan for downtime: Neurodivergent folks often operate in a world not built for them, which can be draining. AuDHD individuals might be juggling constant mental chatter and sensory input, and PDA folks might be on edge about obligations – it’s a lot. Incorporating regular stress-relief and downtime is not just nice, it’s necessary. Exercise is a proven outlet (one AuDHD adult in a survey noted, “Exercise really helps” with clearing the mental jumble). Mindfulness or breathing exercises can help calm that fight-or-flight response. Hobbies that have no productivity goal attached (just pure enjoyment) are great for recharging. And don’t forget the power of stimming or fidgeting to self-soothe if you’re autistic or ADHD – rocking, doodling, pacing, twirling things in your hand, whatever feels good, is totally valid. Make time where there are no demands on you – even an hour of unscheduled “do whatever I want” time each day can reduce the pressure valve.
Seek neurodivergent-friendly support: If you’re struggling significantly, consider finding a therapist, coach, or support group that gets neurodivergence. A professional who understands both autism and ADHD can help you untangle challenges and develop strategies tailored to your unique brain (and won’t pathologize things like stimming or needing routine). Peer support can be equally valuable – connecting with other Autistic-ADHD or PDA adults, whether online or in person, lets you swap tips and feel understood. Sometimes just hearing “I experience that too” from someone can relieve a huge weight of feeling like you’re the only one.
Strategies for Parents and Teachers (Supporting Neurodivergent Kids)
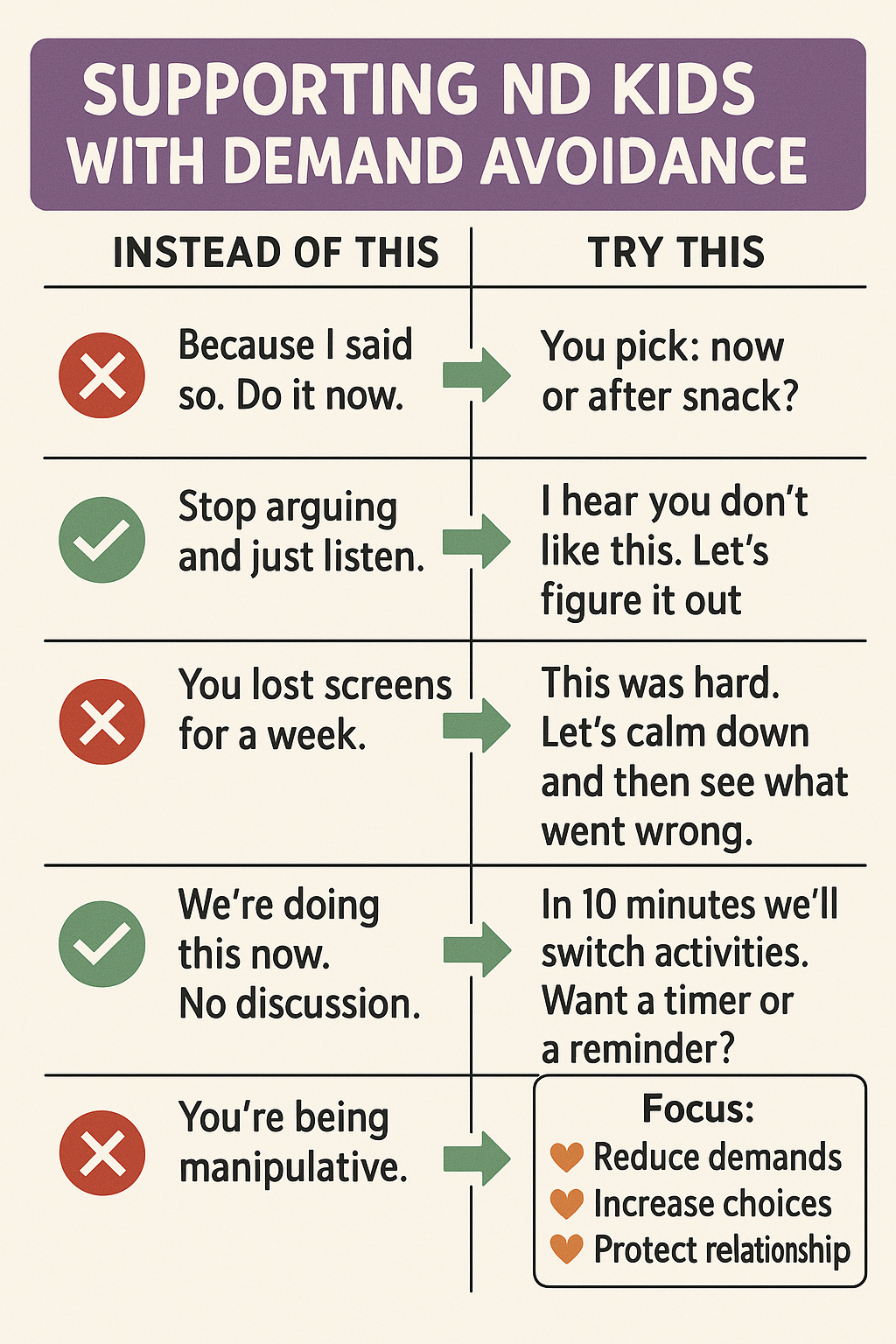
Adopt a collaborative approach: Traditional “because I said so” or strict authoritarian parenting doesn’t usually go over well with PDA kids (or many autistic/ADHD kids, for that matter). Instead of issuing direct orders, invite the child into the process of whatever needs to be done. Offer choices and use negotiation to give them a sense of control. For example, if homework needs to be completed, you could ask, “Which would you like to do first, math or reading?” or “Do you want to do homework before dinner or after dinner?” This way the demand isn’t a one-sided command; the child has some agency. In a classroom, instead of “Take out your textbook now,” a teacher might say, “I’m going to set a timer – let’s see how many problems we can solve in 5 minutes!” to make it a joint challenge. By flattening the adult-child hierarchy a bit and working with rather than against the child, you reduce their instinct to resist.
Motivation over confrontation: Discover what genuinely motivates the child and use that as your leverage, rather than getting into power struggles. If a kid with PDA won’t get dressed in the morning, find something they do want – “We can play your favorite song while we get dressed” or “If you get dressed, we’ll have five minutes to play with your Lego before leaving.” Focus on what interests them or what they stand to gain, rather than the bare demand. With autistic/ADHD kids, incorporate their special interests into tasks: a child obsessed with Pokémon might do math if you frame problems about Pikachu, for instance. Also, use positive reinforcement generously for any cooperation – praise their efforts specifically (“I noticed you started your homework even though you didn’t feel like it – that was really responsible!”). Just be cautious with very competitive or reward-focused systems for PDA kids; if they feel manipulated by sticker charts or if a reward seems to turn an activity into a demand, it could backfire. Sometimes low-key encouragement and making tasks fun works better than obvious reward/punishment with these kids.
Pick your battles (reduce unnecessary demands): Parents and teachers, it’s helpful to triage which demands are truly non-negotiable and which you can relax. Constantly saying “No” or “Do this now” all day long sets up a combative dynamic and fills the child’s “demand bucket” to overflowing. Ask yourself, “Does this have to be a demand?” For example, does it matter if the child wears mismatched socks? Probably not – that could be a choice you let them have. Do they have to do their homework right at 4 PM, or can the schedule be flexible if they’re not in the right headspace until later? By lowering the overall number of demands, you’re conserving the child’s capacity to handle the essential ones (like safety rules, taking medicine, etc.). In practical terms, this might mean allowing more minor negotiables (“Okay, you don’t want to eat your peas – would you rather have carrots or no veggie tonight? Fine.”) so that when a non-negotiable comes up (“You must hold my hand in the parking lot”), the child isn’t already in rebellion mode. Reducing demands isn’t “letting the child run the show”; it’s strategically avoiding unnecessary battles so you can win the important ones.
Use indirect communication: The way you phrase things can significantly affect how a demand is received. PDA children, in particular, are often language-sensitive – direct orders can immediately raise their defenses. Try phrasing things more indirectly or as questions. Instead of “Clean your room now,” you might say, “I wonder what we could do to make your room more comfy? Maybe we could put some of these toys on the shelf. What do you think?” Or use humor and play: “This room looks like a dragon’s den! Should we be brave knights and tame the mess?” Teachers in a classroom might say, “It would be great if everyone could open their books to page 10,” rather than barking an order. Another tactic is speaking as if you need help: “Hmm, I’m not sure how to tie these shoes... Could you show me how you do it?” Such phrasing appeals to a child’s autonomy and often they’ll comply because it doesn’t feel like a demand at all. It feels like they’re choosing to help or participate. Over time, you’ll learn which phrasing your child responds to best – some parents even find success narrating tasks in third person (“The mom robot is picking up toys... will the kid robot join in?” – it sounds silly, but it can turn a demand into play).
Prep for transitions and give warnings: Many autistic and ADHD kids struggle with transitioning from one activity to another. A sudden “Do this now” will likely meet resistance or meltdown. Instead, preview and countdown transitions. Use timers or visual schedules if possible (“In 10 minutes, we’ll need to start homework. Here’s a timer.” then “5 minutes left...” etc.). For a PDA child, giving them a role in the transition can help: “We need to leave the playground soon. What final thing do you want to do before we go? One more slide or one more swing?” – that way the end of play is their decision to some extent. Visual schedules (with pictures for younger kids) can also help reduce the anxiety of “What’s coming next?” If they see that after lunch is “free time” and then “math time” and then “game time,” it’s not a shock when those moments arrive. Of course, life isn’t always predictable – if something changes (say a favorite activity is canceled), try to cushion it: explain clearly why (“The pool is closed today, so we can’t go swimming – I’m upset too!”) and perhaps offer an alternative choice (“Would you rather go to the park or watch a movie at home instead?”). This helps maintain trust and gives back a bit of control when plans go awry.

Scaffold tasks to build confidence: Often, ND kids have a gap between what they can do (their actual ability) and what they will do under pressure. They might avoid a task because it seems too hard or they’re afraid of failing. Your job is to bridge that gap with scaffolding – support them step by step. Let’s say a child refuses to brush their teeth. Instead of a nightly battle, break it down. First, you brush your teeth next to them and don’t even ask them to do it, just let them watch for a few days. Then maybe let them play with the toothbrush with no expectation. Next, you brush their teeth for them in a fun way (maybe while they hum a song). Then you do it together – you brush yours while they brush theirs, maybe in front of a mirror making silly faces. Gradually, you remove your involvement as they build confidence. This principle can apply to homework (do one problem together, then let them try one), to chores (start the task for them, then invite them to finish). Celebrate and praise any small step they take. The goal is to build their sense of competence and reduce the fear that often underlies demand avoidance. It can be tedious at first, but once they feel “I can do this (and it’s not so bad)”, their avoidance usually lessens.
Adjust expectations and be flexible in outcomes: This is especially relevant for teachers but also parents. Sometimes a neurodivergent child can complete a task, but how they do it might be unconventional – and that’s okay. For example, a child with PDA might only do their writing assignment if they can type on a computer instead of handwriting (fine, the learning goal of writing can still be met). Or an autistic/ADHD child might fidget or stand at their desk during a lesson – if they’re still learning, that behavior might be acceptable even if it looks different from other kids. Don’t insist on a “one right way” if the objective can be achieved through an alternative. Similarly, you might “taper your expectation” of compliance: maybe the child won’t clean their whole room, but they’ll put toys in the bin while leaving clothes on the floor – that’s progress. A neurodiverse child may do things differently, and adapting to that rather than labeling it disobedience can reduce a lot of conflict.
Support emotional regulation and independence: Kids with AuDHD might experience big emotions (from ADHD impulsivity or autistic emotional intensity), and PDA kids obviously have anxiety spikes around demands. Teaching and modeling emotional regulation is huge. This can include showing them calming techniques (deep breathing, counting to 10, squeezing a stress ball) when they start getting frustrated. It also involves you staying as calm as possible during their episodes – your calm is their anchor. Afterwards, when everyone is regulated, gently discuss what happened: “It seemed like putting on shoes made you upset. Can you tell me what bothered you about it? Maybe we can find a way to make it easier.” Over time, help them name their feelings and signals (“My tummy feels tight when I have to do homework – that might be worry.”). Consider engaging a child therapist or occupational therapist if emotional meltdowns are frequent; professionals can do targeted work on coping skills and flexibility (for example, some therapies use games to practice flexibility and turn-taking, which can indirectly help with demand avoidance). Also, explicitly teach adaptive skills for independence when possible – like cooking, self-care, etc. Often ND kids lag in adaptive skills not because they can’t do them, but because they’ve been avoiding demands for so long that others do things for them. Encourage and enable them to take on small responsibilities in a supported way, to build confidence and reduce over-reliance on adults. This might mean creating a visual checklist for morning routines so they can do it themselves, or letting them make choices about their schedule so they feel ownership. The more they feel capable and in control of their own life, the less threatening each new demand will seem.
Empathy and patience over punishment: Remember that the child isn’t giving you a hard time on purpose – they are having a hard time. When faced with a defiant or avoidant behavior, try to see the fear or confusion underneath. Responding with empathy (“I see this is really upsetting for you”) doesn’t mean you give in to every demand, but it validates their feelings. Often, just feeling understood can de-escalate a situation. Avoid harsh punishments for demand-avoidant behavior – if a child could calmly comply, they would. Consequences might be needed sometimes (for example, if they hurt someone during a meltdown, they should repair that), but punitive approaches like yelling, taking away all privileges, etc., usually just increase anxiety and damage trust. Instead, focus on problem-solving together once calm: “What can we do differently next time?” and praising any effort they make. Building a strong, trustful relationship with the child is like creating a safety net – they learn that you’re on their side, not just an enforcer. Over time, this can reduce the intensity of avoidance, because the child doesn’t immediately assume a demand equals an adversarial battle. Your calm consistency and love, even when they’re at their worst, sends the message that they’re safe and accepted, which can gradually help them handle challenges better.

Reflection Journal Prompts
Self-reflection can help you internalize what you’ve learned and tailor it to your own situation. Here are some journaling prompts to consider, whether you’re a neurodivergent adult exploring your own patterns or a parent/teacher trying to better understand your child or student:
For Neurodivergent Adults: Think of a recent time when you found yourself avoiding a task or responsibility that you knew was important. What feelings came up at the thought of doing it (e.g., anxiety, fear of failure, anger at being told what to do)? Can you identify whether it was the nature of the task, the way it was presented, or something internal (like your energy level or mood) that made you want to nope out? Write about one small change that could make that task feel more doable — for example, breaking it into a tiny step, doing it at a different time of day, or pairing it with something pleasant.
For Parents/Teachers: Recall a situation when the child resisted a demand and things went badly (a meltdown, an argument, or a stalemate). Describe the sequence from the moment the demand was made to the reaction and aftermath. What do you think was the trigger for the child’s avoidance? Try to put yourself in the child’s shoes: what might they have been thinking or feeling at that moment (“This is too scary/overwhelming/boring,” etc.)? Now brainstorm how you might present the same demand differently in the future. Could offering a choice, giving more warning, or changing the environment make a difference?
List out some of the strengths and interests of yourself (if you’re the ND adult) or your child. Next to each, jot an idea for how that strength or passion could be used to tackle a challenge. For instance, if the person has a special interest in art, could drawing or visual aids be integrated into learning a tough subject? If they have a great sense of humor, can you turn a chore into a silly game? This exercise helps shift focus from deficits to creative solutions, leveraging what the neurodivergent person naturally does well.
Write about a time when having autism or ADHD (or both) actually helped you or your child in an unexpected way. Did hyperfocus enable a big achievement or creative project? Did a need for routine create helpful structure that others benefited from? Did questioning authority (PDA-style) lead to spotting an unfair rule that needed changing? Reflecting on these moments can build a more balanced perspective – neurodivergence comes with challenges, but also with valuable insights and strengths.
If demand avoidance is a big issue in your life, describe what your “ideal low-demand day” would look like. What routines, environment, and supports would make you (or your child) feel safe and in control while still getting important things done? Once you paint that picture, see if there’s one element of it you can actually implement in real life, even in a small way. For example, if the dream is a slow-paced morning with no rushing, maybe you can adjust bedtime/wake-up time to allow a gentler morning routine. Use your ideal scenario as inspiration for practical changes.
Consider writing a short, compassionate note to yourself or to your child about these challenges. Acknowledge the hard work you’re doing to cope or to help. For example: “Dear Self, I know I get overwhelmed when people put demands on me. It’s not because I’m weak; it’s because my brain interprets pressure differently. I’m proud of myself for getting through yesterday – even though I panicked about that meeting, I still showed up for it. That’s a win.” Or, as a parent to a child: “Dear [Child’s Name], I see how hard you try every day. I know getting through school and homework is extra tough for you, but you are so resilient. I love how creative and funny you are, and we will keep figuring out ways to make things work for you.” Writing in this kind, understanding tone can shift your mindset from frustration to empathy.
By exploring these prompts, you may uncover new insights about how AuDHD or PDA affects daily life and how you can adapt with greater empathy for yourself or your loved one. Remember, there’s no one-size-fits-all in the neurodivergent world. It’s all about understanding individual patterns and needs, and growing together with that knowledge.
Sources
American Psychiatric Association – “When Autism and ADHD Occur Together,” APA Blogs (July 17, 2025)psychiatry.orgpsychiatry.orgpsychiatry.org.
Farahimanesh, S. – “What is AuDHD? Five Key Points to Understand When Someone Has Both Autism and ADHD,” Evergreen Memory (July 17, 2024)evergreenmemory.comevergreenmemory.com.
Russell, G. – “ADHD and Autism: How They’re Related and Why It Matters,” Neurodivergent Insights (2023)neurodivergentinsights.comneurodivergentinsights.com.
Miller, C. & Martin, C. – “Pathological Demand Avoidance (PDA) in Kids,” Child Mind Institute (last reviewed Oct 29, 2025)childmind.orgchildmind.org.
Gerlach, J. – “What Does Pathological Demand Avoidance Look Like in Adults?” Psychology Today (Aug 13, 2024)psychologytoday.compsychologytoday.com.
National Autistic Society (UK) – “Demand Avoidance: What is it and Why Does it Happen?” (2023)autism.org.ukautism.org.uk.