Do I Have AuDHD?
What AuDHD traits actually look like, why they get missed, how they can differ across gender presentation, and how to tell the difference?

There is a specific kind of ache that lives inside the question, “Do I have AuDHD?”
Not curiosity, exactly. More like grief with a flashlight.
Because usually that question does not show up out of nowhere. It shows up after years of feeling off-script. After a lifetime of being “too much” in one room and “not enough” in another. After realizing that some of your struggles do not fit neatly into the autism box or the ADHD box, but somehow both are sitting there on the floor of your brain, throwing glitter, losing the instructions, and refusing to make eye contact.
And for a lot of us, especially adults, especially women, especially people socialized to be agreeable, observant, high-masking, and “good,” the question is not, “Could I possibly be neurodivergent?”
The question is more like:
How did no one catch this sooner?
Why do I look capable and feel like I’m drowning?
Why am I both pattern-loving and chaos-prone?
Why do I need sameness and also feel like I’ll die of boredom?
Why do I seem socially perceptive and socially exhausted at the same time?
That tension right there? That internal tug-of-war? That is part of why AuDHD can feel so confusing from the inside and so invisible from the outside.
Autism and ADHD are both neurodevelopmental conditions, meaning they begin in development and reflect differences in how the brain processes information, attention, behavior, sensation, and social experience. They also commonly co-occur. Research has consistently shown that autism and ADHD overlap at high rates, and newer large-scale data continue to show elevated ADHD rates in autistic people well into adulthood.
So let’s talk about it clearly. No nonsense. No TikTok astrology disguised as neuroscience. Just the messy, human, research-informed truth.
First: what people mean when they say “AuDHD”
“AuDHD” is not usually a formal diagnostic label in itself. It is a community term people use to describe co-occurring autism and ADHD. In plain English: both sets of traits are present, both affect functioning, and the interaction between them creates a profile that is often more complicated than either condition alone.
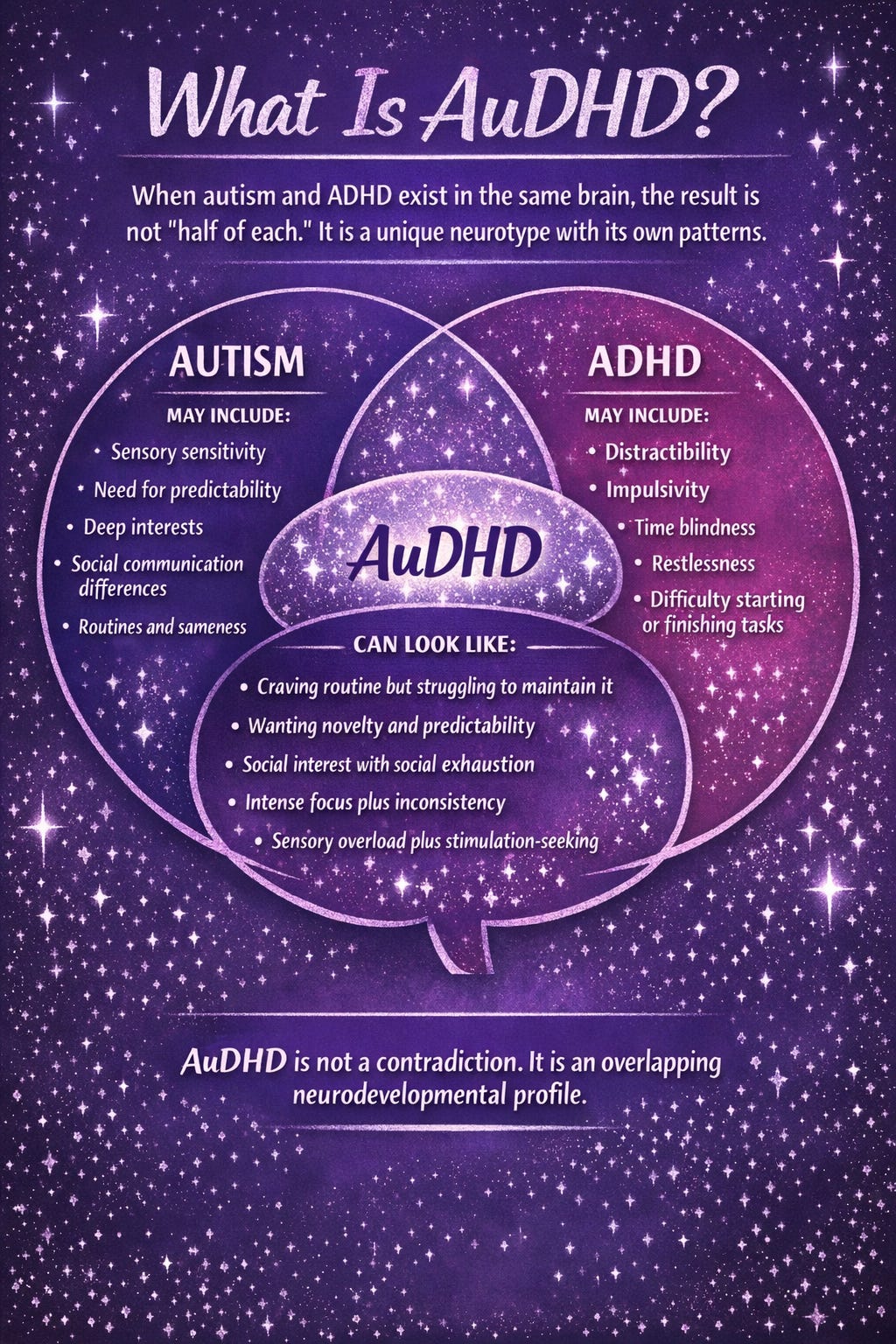
That matters, because a lot of people assume autism and ADHD cancel each other out. They do not. They can actually create a very specific push-pull dynamic.
You may crave routine but fail to maintain it.
You may need predictability but impulsively change everything.
You may deeply want connection but become overwhelmed by the mechanics of socializing.
You may be highly imaginative and mentally restless, while also needing intense sameness around food, clothing, interests, or environment.
You may read some social patterns brilliantly and miss others entirely.
You may have a fast, idea-rich brain that is also wiped out by sensory input and transition demands.
That is one reason AuDHD gets missed: it does not always look clean. It can look contradictory. But contradictory does not mean made up. It means multiple brain systems are involved.
What “neurotypical” vs. “neurodivergent” actually means
Let’s clear something up, because the internet has been doing internet things.
“Neurotypical” does not mean “perfectly mentally healthy, socially polished, productive, regulated, and serene like a woman in a yogurt commercial.”
It means a person’s brain development and behavioral profile falls closer to expected population norms, especially in areas like social communication, attention regulation, sensory processing, and behavioral flexibility.
“Neurodivergent” is a broader umbrella term often used for brains that diverge from those typical patterns—autism, ADHD, dyslexia, dyspraxia, Tourette’s, and more. It is not a medical diagnosis by itself. It is a descriptive framework. And it is useful because it shifts the conversation away from moral judgment and toward brain differences plus environment fit.
The important part is this:
everyone has some traits.
Lots of people get distracted. Lots of people like routines. Lots of people miss social cues sometimes. Lots of people get overwhelmed.
The question is not whether you have a few relatable traits.
The question is whether there is a persistent developmental pattern across time that meaningfully affects how you function, adapt, recover, and move through the world.
For autism, the core pattern involves social communication differences and restricted/repetitive patterns of behavior, interests, or sensory experience, beginning in development. For ADHD, the core pattern involves persistent difficulties with attention regulation, impulsivity, and/or hyperactivity that are developmentally inappropriate and impairing. Both can look different across people, and both can be missed when someone has learned to compensate.
So the real difference is not:
“Do I ever do this?”
It is more like:
“Has this been a pattern for most of my life?”
“Does it show up across settings?”
“Does it cost me more effort than people realize?”
“Am I functioning, or am I compensating?”
“Is this a quirky preference, or is this a nervous system reality?”
That last one matters a lot.
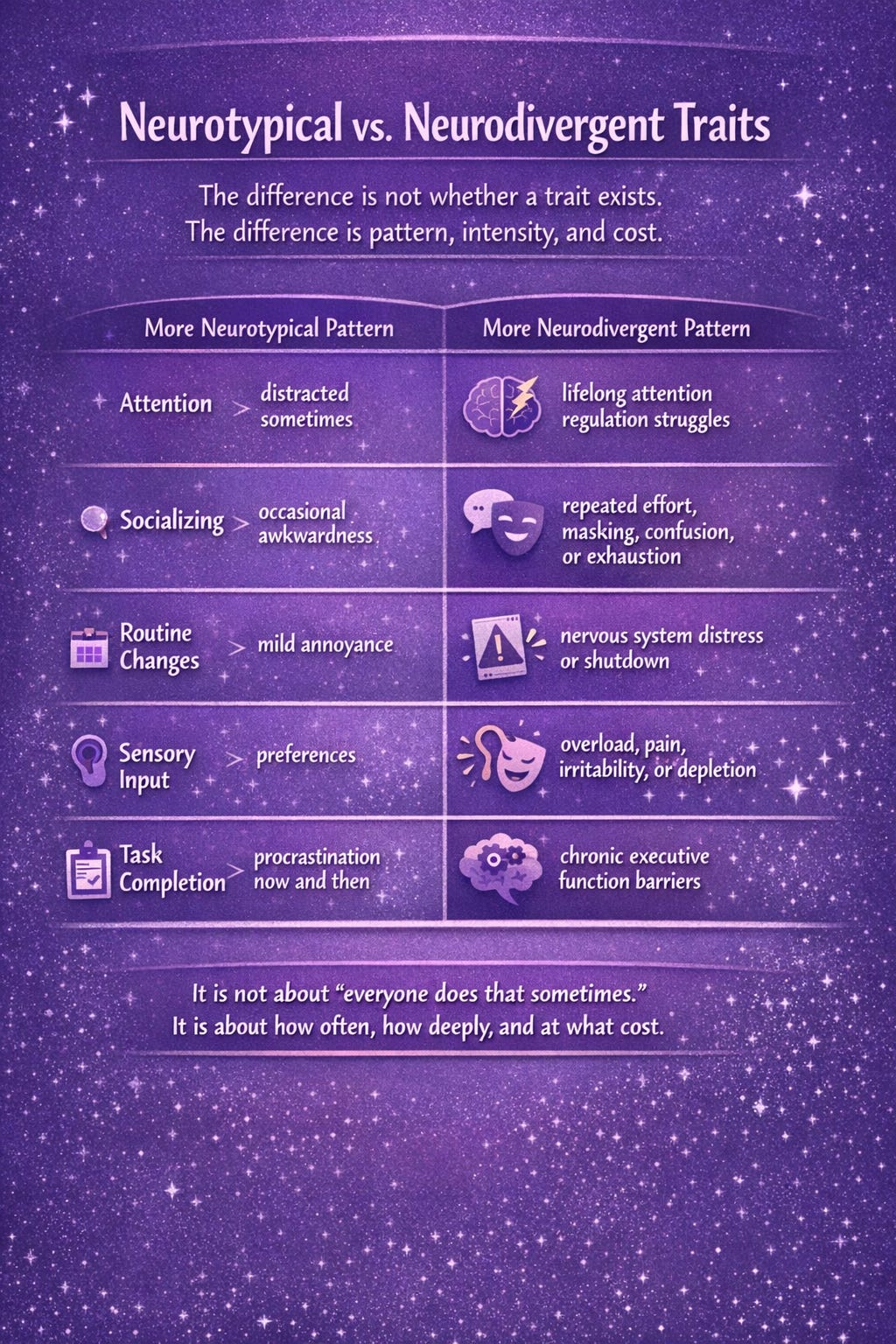
What neurotypical traits often look like
Not in a robotic, diagnostic-manual way. In real life.
A more neurotypical profile often means:
You can adapt to changing plans without a massive internal crash, even if you are annoyed.
You might dislike some textures, sounds, or social situations, but they do not repeatedly hijack your nervous system.
You might procrastinate or get distracted, but there is not a lifelong pattern of chronic disorganization, time blindness, task paralysis, or impulsive inconsistency that keeps punching holes in your life.
You usually do not need to script conversations, study people to “do socializing correctly,” or recover from ordinary interaction like you just finished a hostage negotiation.
You may have preferences, habits, and personality traits, but they generally do not create the same developmental and functional pattern seen in autism or ADHD.
Again, neurotypical does not mean easy life. It just means the brain is, on average, more aligned with the social and cognitive demands the environment expects.
What neurodivergent traits often look like
This is where it gets trickier, because neurodivergence is not one aesthetic. It is not all visible. It is not always loud. It is not always childhood boy running into furniture and licking drywall energy.
Sometimes it looks like:
being chronically “too sensitive” to sound, clothing, interruption, lighting, or chaos
needing sameness, structure, or special interests to feel regulated
intense justice sensitivity or deep pattern recognition
difficulty with transitions, shifting attention, or changing gears
chronic forgetfulness, lateness, losing things, or inconsistent performance
social exhaustion despite caring deeply about people
masking, mirroring, rehearsing, overexplaining, or people-pleasing to survive socially
burnout after years of holding it together externally
feeling like daily life takes way more invisible labor than it seems to take for other people
What makes it neurodivergent is not just the presence of traits. It is the pattern, intensity, developmental history, and cost.
A person can look “fine” and still be using ten times the cognitive energy to appear fine. That is especially true in high-masking autistic people and in people with inattentive ADHD, who are often missed because they are not disrupting other people enough to get noticed.
Which is, frankly, one of the darker little jokes of the diagnostic system: if your distress is neat, internal, quiet, or useful to others, it may go untreated for years.
Why AuDHD feels so contradictory from the inside
Because autism and ADHD can pull in opposite directions.
Autism often leans toward predictability, pattern, depth, sameness, and reduced novelty load. ADHD often leans toward novelty-seeking, stimulation-seeking, impulsivity, and inconsistent executive control. Both are associated with executive function difficulties, but not always in identical ways. Reviews continue to support overlap in executive function challenges across ADHD and autism, especially in areas like cognitive flexibility, inhibition, working memory, and self-regulation.
So an AuDHD brain may say:
“I need structure.”
and also
“I hate this structure now.”
“I want a plan.”
and also
“I refuse the plan on principle.”
“I desperately need low sensory input.”
and also
“I am understimulated and climbing the walls.”
“I want friends.”
and also
“I need everyone to stop talking immediately.”
That does not mean you are dramatic. It means multiple systems are competing for the steering wheel
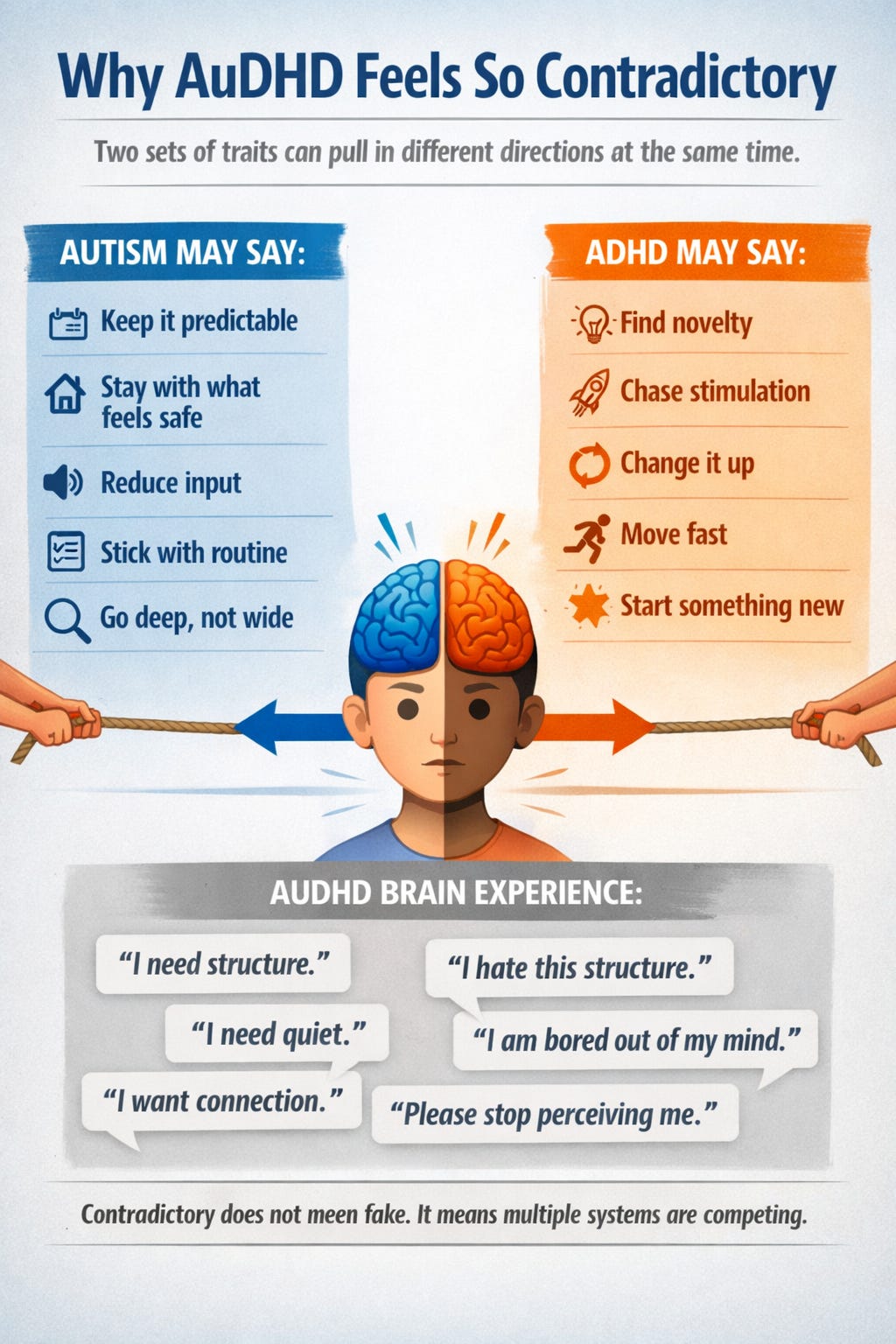
.
Why our brains are like this
This is where neuroscience helps, not because it makes anyone more valid, but because it can reduce shame.
Autism and ADHD are neurodevelopmental. That means the differences emerge during brain development and reflect variations in neural circuitry, genetic liability, information processing, and developmental timing. Research continues to support substantial genetic overlap between autism and ADHD, alongside meaningful differences too. In other words, these are not identical conditions, but they are not strangers either. They share part of the wiring diagram.
Broadly speaking, the brain systems involved can include:
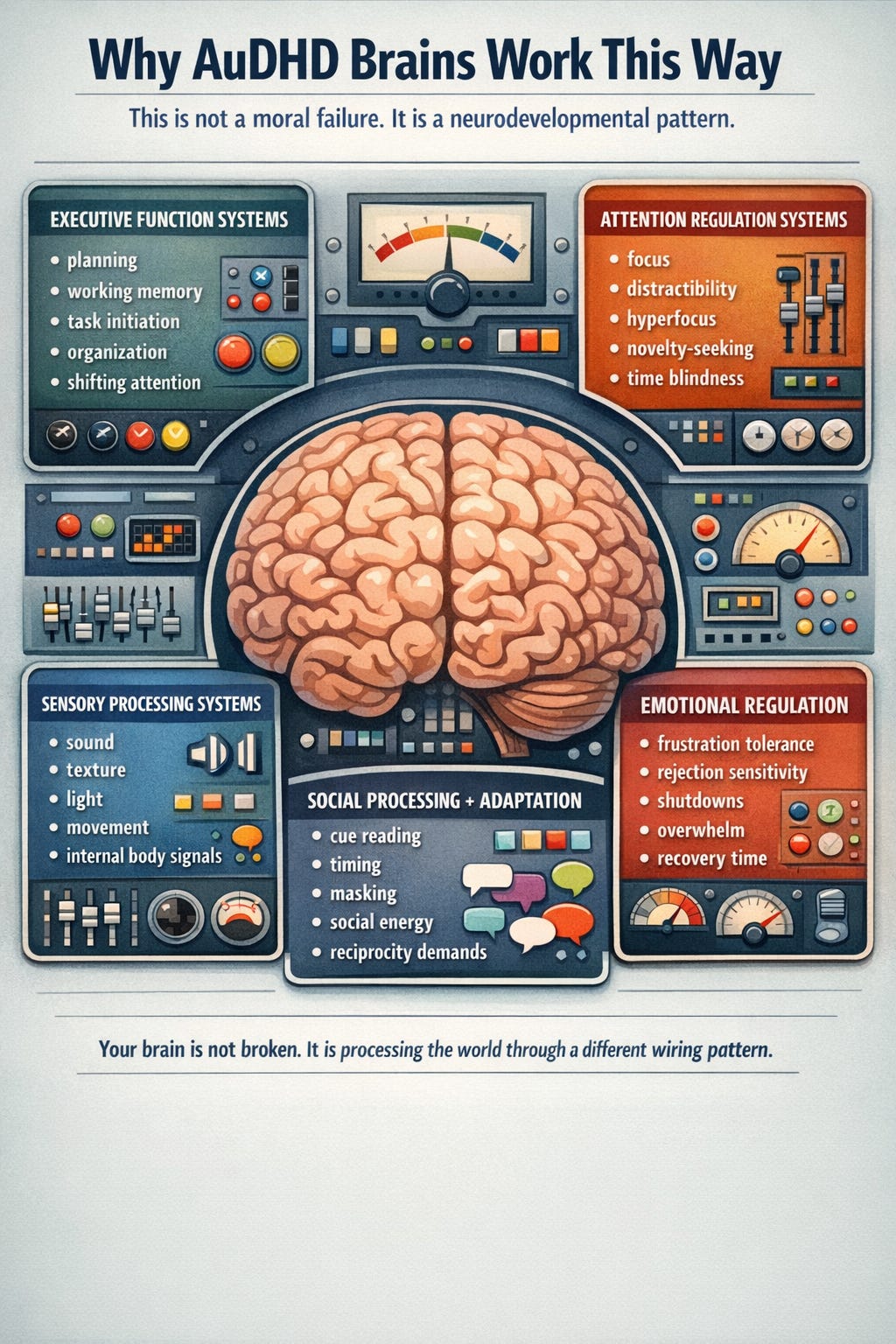
Executive function networks
These help with planning, working memory, inhibition, shifting attention, and self-monitoring. When these systems are taxed, life becomes a constant game of “I know what to do, why can’t I reliably do it?”
Attention regulation systems
ADHD is not an inability to pay attention. It is a difficulty regulating attention in line with demand. That can mean distractibility, hyperfocus, inconsistent performance, time blindness, and difficulty initiating or sustaining effort on low-interest tasks.
Sensory processing and salience systems
Autistic people often experience differences in how sensory information is filtered and prioritized. The world may feel too loud, too bright, too scratchy, too fast, too much. The nervous system is not being “dramatic.” It is processing input differently. CDC notes that autistic people can show different ways of learning, moving, and paying attention, alongside sensory and behavioral differences.
Reward, novelty, and motivation systems
ADHD is strongly tied to differences in how the brain responds to reward, delay, stimulation, and effort. This is one reason “just try harder” is such useless advice. It is not a character problem. It is a regulation problem.
Social processing and adaptation systems
Autistic people may process social information differently—not necessarily less deeply, but differently. That can affect timing, reciprocity, interpretation of cues, and how exhausting social participation feels. Some autistic people use masking or camouflaging strategies to mimic expected social behavior, which can hide distress and delay identification.
So no, your brain is not “broken.”
But it may be built around a different set of priorities, thresholds, and processing routes than the world expects.
And when the world keeps grading you with the wrong answer key, shame starts to grow in places science should have reached first.
Gender presentation differences in kids: why so many girls and gender-diverse kids get missed
Let’s say the quiet part out loud: much of the older diagnostic literature was built around more stereotypically male presentations.
That does not mean autism and ADHD are “male conditions.” It means the recognition systems were biased toward the traits adults were most trained to notice.
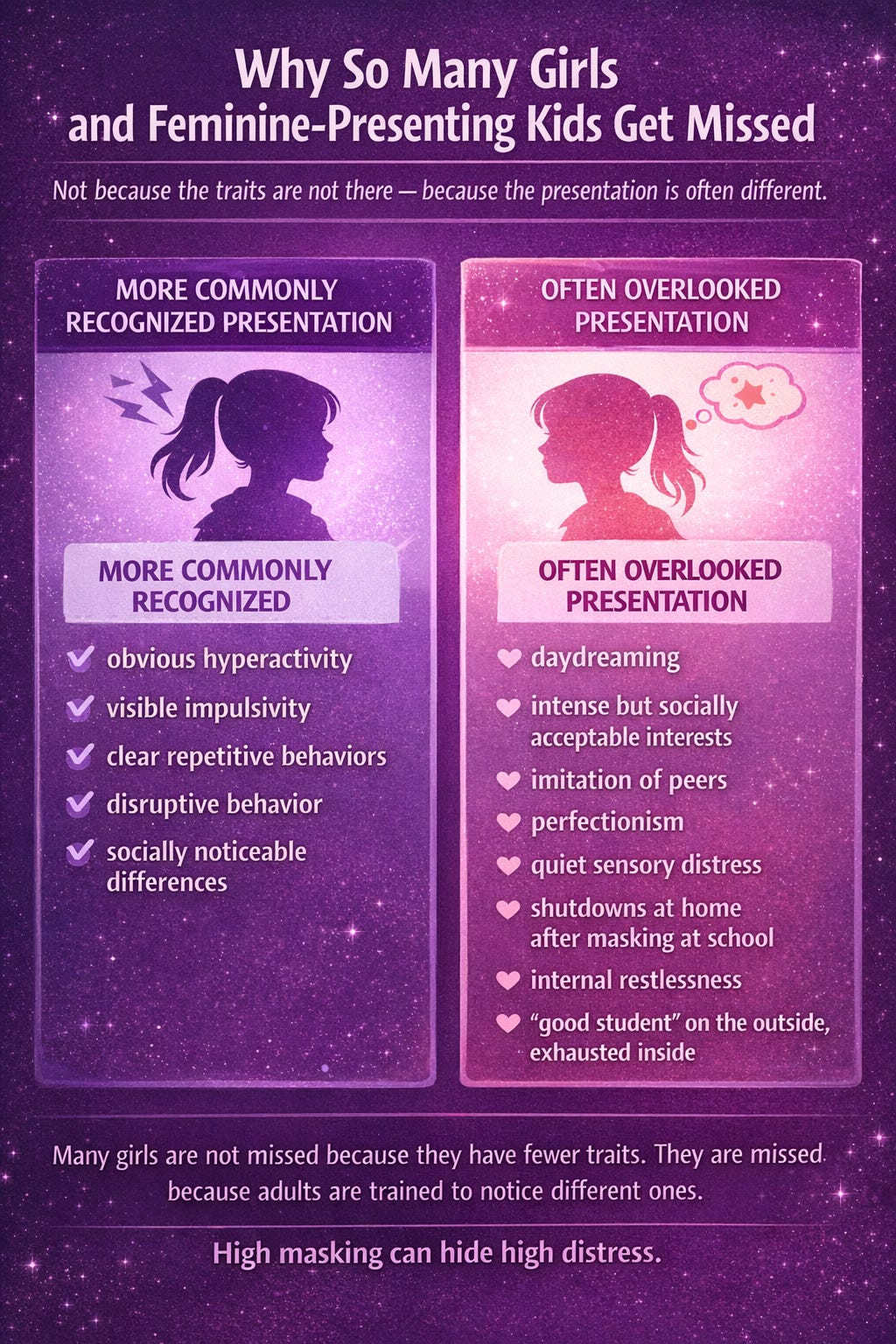
In kids, boys are more likely to be flagged when traits are externalized: visible hyperactivity, disruptive behavior, obvious repetitive behavior, more stereotypically noticeable social differences. Girls and some gender-diverse kids may present differently or may be more likely to camouflage. CDC notes that autism identification still differs by sex, and one reason may be differences in how signs and symptoms show up and are recognized.
In autistic girls or feminine-presenting kids, traits may look more like:
intense interests that appear socially acceptable, like books, animals, celebrities, psychology, art, or school subjects
imitation of peers and strong observational learning
one or two close friendships rather than obviously absent interest in peers
strong social desire but confusion about the rules underneath interaction
perfectionism, rigidity, shutdowns, or internal distress more than visible “behavior problems”
sensory issues framed as “picky,” “sensitive,” “dramatic,” or “anxious”
high masking at school and meltdowns at home
In girls with ADHD, traits may look more like:
daydreaming
zoning out
chronic disorganization
emotional intensity
talkativeness
internal restlessness instead of obvious motor hyperactivity
overcompensating academically while quietly falling apart
being labeled careless, messy, lazy, moody, or scattered instead of recognized as ADHD
Recent and current literature continues to point to delayed diagnosis in females, in part because inattentive and internalized presentations are easier to miss, and because masking can hide distress.
So the little girl who seems “fine” because she is quiet, bright, compliant, anxious, and exhausted?
She may not be fine.
She may just be socially expensive.
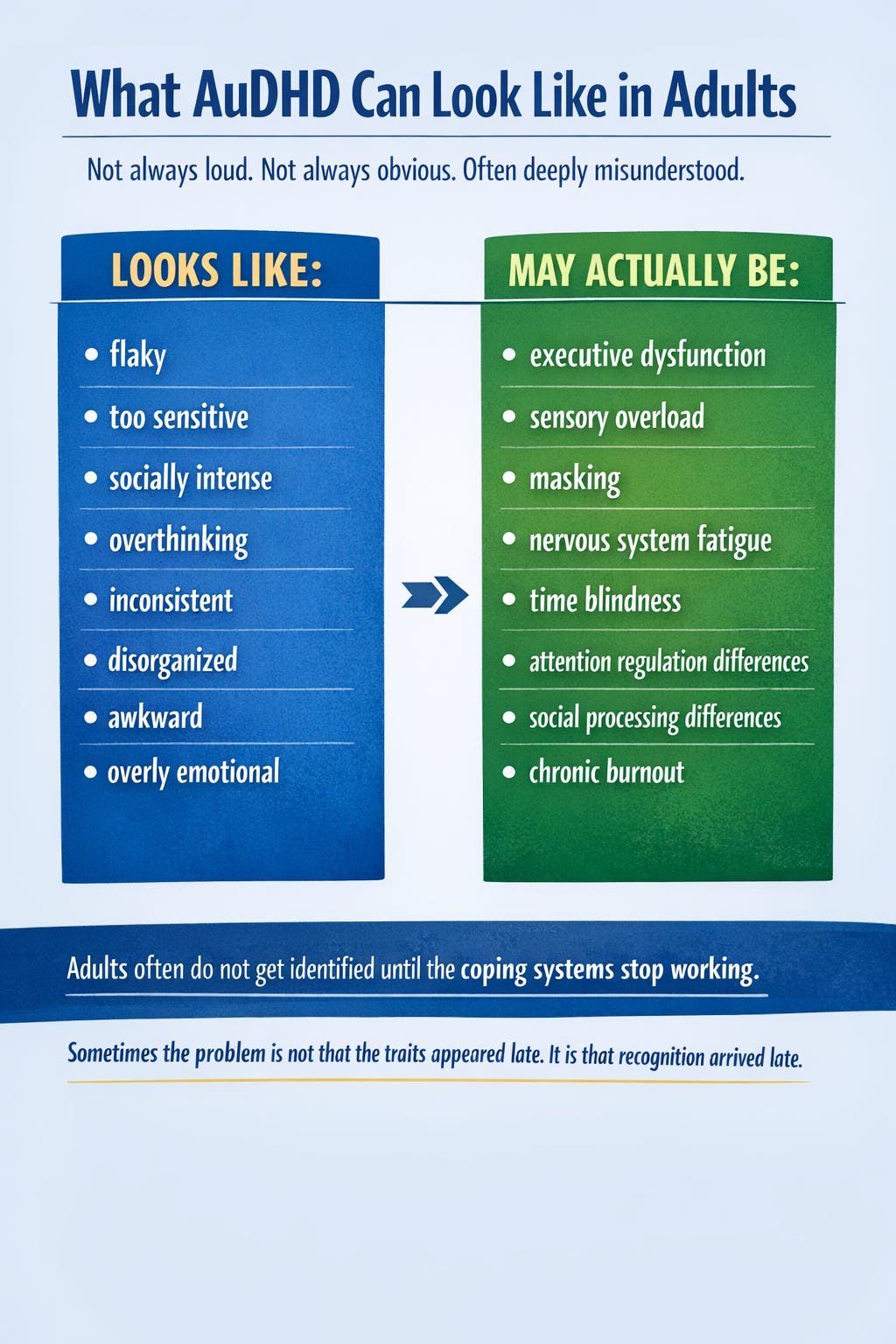
Gender presentation differences in adults: why so many people realize it later
Adult identification often happens after the scaffolding collapses.
Childhood structure helped. Intelligence helped. People-pleasing helped. Fear helped. Being “the responsible one” helped. But adulthood is where invisible support gets ripped away and suddenly the person is expected to self-manage time, food, money, emotions, relationships, work, admin, sensory load, and identity like it is no big deal.
For many adults—especially women and gender-diverse people—AuDHD is finally considered only after burnout, parenting, career overload, relationship strain, hormonal changes, or a child’s diagnosis makes the pattern impossible to ignore.
In adults, autism may show up less as the stereotype of “doesn’t want people” and more like:
wanting connection but needing enormous recovery time
scripting conversations
forcing eye contact
overanalyzing tone, facial expression, and social rules
missing subtext while still being highly perceptive in other ways
deep sensory and routine needs
intense interests, deep dives, and identity-level attachment to certain topics
chronic masking followed by collapse
ADHD in adults may show up less as “can’t sit still” and more like:
procrastination with panic-powered completion
chronic overwhelm
starting everything
finishing selectively
missed deadlines
forgetting what you were doing mid-task
emotional impulsivity
interrupting
difficulty shifting gears
a brain that is either overclocked or buffering
And in AuDHD adults, those patterns can stack in deeply confusing ways:
you may be socially skilled and socially exhausted, organized in one domain and feral in another, hyperverbal yet shutdown-prone, flexible in a crisis and rigid about tiny daily rituals.
That is not inconsistency in the moral sense.
That is a neurodevelopmental profile colliding with life demands.
So… how do you tell the difference?
This is the part people want in a neat checklist. I regret to inform us all that brains are rude and rarely do neat.
But here are the big clues.
1. Look for a developmental pattern, not a mood
AuDHD traits are not something that appears out of nowhere at age 34 because you got busy and bought a planner. These are developmental conditions. The presentation may shift over time, but the underlying pattern usually has roots in childhood, even if it was missed or mislabeled.
Ask:
Were there signs early on, even subtle ones?
Was I “gifted but struggling,” “sensitive,” “dramatic,” “spacey,” “rigid,” “bossy,” “shy,” or “too intense”?
Did I seem mature in some ways and behind in others?
Did I have big feelings, sensory issues, friend confusion, or chaotic attention patterns early?
2. Look at cost, not just appearance
Can you do the thing, or can you do the thing by setting your nervous system on fire?
This is huge.
A lot of high-masking people say, “But I can socialize,” or “I can keep up at work,” or “I can make eye contact.”
Okay. And what does it cost?
Masking and camouflaging can hide autistic traits externally while increasing stress internally. Research has linked camouflaging with greater psychological strain, and girls may use these strategies more often.
If your competence is held together by panic, rehearsal, burnout, and recovery debt, that matters.
3. Look for cross-setting patterns
Is it only happening in one toxic job? One relationship? One semester? Then maybe environment is the main issue.
Does it happen at home, at school, at work, in friendship, in routines, in sensory environments, in task initiation, in transitions, in recovery? That points more toward a broader neurodevelopmental pattern.

4. Look for contradiction clusters
This is classic AuDHD territory.
Do you:
crave routine and resist it?
need novelty and hate disruption?
want closeness and hide from contact?
hyperfocus for hours and still lose essential details?
notice patterns intensely and miss practical steps?
feel emotionally intense but struggle to identify what you need in the moment?
That tension does not prove AuDHD, but it is often a clue.
5. Rule out “just anxiety” as the whole story
Anxiety can absolutely mimic or intensify attention, sensory, and social difficulties. Same with trauma, depression, sleep problems, OCD, and chronic stress.
But sometimes anxiety is not the original engine. Sometimes it is the smoke from a brain that has spent years trying to survive misunderstood neurodivergence.
That distinction matters.
If the anxiety showed up because you were always missing cues, forgetting things, getting in trouble, being overwhelmed, overcompensating, or trying to perform normalcy—then anxiety may be a co-occurring layer, not the whole explanation.
6. Ask whether the traits are trait-level, not trend-level
Social media has made everyone suspicious of themselves, which is understandable. But having three relatable memes and a deep love of noise-canceling headphones does not automatically equal AuDHD.
The difference is usually:
persistence
pervasiveness
impairment
developmental history
internal effort
nervous system cost
That is the boring clinical answer, but boring answers are often the truest.
What AuDHD can look like compared with ordinary human variation
A neurotypical person may dislike small talk.
An autistic person may find the entire choreography of social interaction effortful, opaque, or draining in a repeated, developmental way.
A neurotypical person may procrastinate boring tasks.
A person with ADHD may experience chronic task initiation problems, time blindness, inconsistent activation, and repeated functional fallout.
A neurotypical person may love routines.
An autistic person may rely on sameness, predictability, and reduced uncertainty as part of nervous system regulation.
A neurotypical person may get distracted when stressed.
An ADHD brain may show a lifelong pattern of attention dysregulation, not just situational overload.
A neurotypical person may feel socially awkward sometimes.
An autistic person may spend years consciously studying, scripting, imitating, and masking social behavior.
The line is rarely “never vs always.”
It is more like occasional human trait vs enduring nervous system pattern.
Why many people doubt themselves anyway
Because stereotypes are loud and lived experience is subtle.
People doubt themselves because:
they made decent grades
they had friends sometimes
they can make eye contact
they are empathetic
they are verbal
they are successful on paper
nobody noticed
someone told them they were “too smart” to be autistic
someone told them ADHD would have been obvious
they internalized the idea that suffering only counts if it is visible
Meanwhile, the science has been moving. Diagnostic systems have gotten better at recognizing that autism and ADHD can present differently across sex, gender presentation, age, cognitive profile, and masking style. But the public stereotype still lags behind like Internet Explorer in 2009.
So a lot of adults are looking backward and realizing:
“Oh. It was not that I had no signs.
It was that everyone was looking for a different costume.”
A very important note: self-recognition matters, but assessment can still help
Self-reflection is valid. Community language can be life-saving. Recognizing yourself in a pattern can be the first breath after years underwater.
And also, a thorough assessment can be useful—especially when you want more clarity around autism, ADHD, anxiety, trauma, OCD, learning differences, sensory processing, or other overlapping conditions. NICE guidelines for autism in children and adults emphasize careful assessment because presentation varies and overlapping conditions can complicate recognition.
So no, you are not broken for asking.
And no, asking does not automatically mean yes.
But it does mean the question deserves more respect than “everyone does that.”
Because no. Everyone does not do that in the same way, for the same reasons, at the same intensity, with the same cost.
Tips if you’re wondering whether you have AuDHD
1. Start collecting patterns, not just traits
Instead of listing isolated quirks, write down recurring themes:
attention regulation
sensory overwhelm
friendship patterns
transitions
task initiation
recovery time
rigidity vs impulsivity
masking
burnout
shutdowns/meltdowns
childhood patterns
Pattern-recognition is gold here. One trait can mean many things. A cluster tells a story.
2. Ask, “What looks easy from the outside but costs me dearly inside?”
This question cuts through masking fast.
Maybe you can attend the gathering.
But do you need two days to recover?
Maybe you can finish the work.
But only through panic and self-erasure?
Maybe you seem socially smooth.
But only because you studied everyone else like it was a final exam?
Cost matters.
3. Look back at childhood through a broader lens
Not just, “Was I hyper?” or “Did I line up toys?”
Ask:
Was I called sensitive, intense, bossy, shy, scattered, dramatic, gifted, lazy, rigid, emotional, forgetful, or too much?
Did I copy other kids to fit in?
Was I exhausted after school?
Did I struggle more at home than people saw outside?
Did routines, interests, or fairness matter deeply to me?
Did I have uneven skills—advanced in some ways, struggling in others?
4. Pay attention to sensory life
Sensory issues are often one of the clearest clues people minimized for years.
Notice:
sound tolerance
clothing/texture needs
lighting sensitivity
food rules or aversions
movement needs
nervous system crashes after crowded or chaotic environments
That is not “being dramatic.” That is data.
5. Separate shame from evidence
A lot of adults cannot see their traits clearly because shame has been narrating the whole movie.
You may think:
“I’m lazy.”
But the evidence may say task initiation impairment.
You may think:
“I’m rude.”
But the evidence may say overload, missed cues, or a different communication style.
You may think:
“I’m flaky.”
But the evidence may say time blindness, working memory strain, and inconsistent executive activation.
Shame is a terrible diagnostician.
6. Learn from high-quality sources, not just personality content
Personal stories matter. They can be healing and illuminating. But pair them with research, guidelines, and clinicians who understand adult, high-masking, and non-stereotypical presentations.
Because the algorithm loves confidence more than accuracy, and unfortunately your nervous system deserves better than that circus.
7. Consider formal evaluation if it would help you
Assessment is not the only path to self-understanding, but it can help with:
clarity
accommodations
treatment planning
support access
language for your experience
ruling in or ruling out overlapping explanations
Especially if you have spent years being treated for anxiety, depression, or burnout without anyone asking why your whole system keeps catching fire.
Reflection journal prompts
Here are prompts you can use privately, in therapy, in coaching, or in the notes app where all major life revelations now apparently live.
Identity and pattern recognition
What traits have I dismissed as “personality” that might actually be part of a neurodivergent pattern?
What has felt different about me for most of my life—not just during stressful periods?
Where do I feel most “normal,” and where do I feel like I’m acting?
Childhood clues
What words did adults use to describe me as a child?
What parts of school felt easy for me, and what parts felt secretly impossible?
Did I cope by overachieving, withdrawing, masking, people-pleasing, or becoming “the funny one,” “the smart one,” or “the quiet one”?
Social experience
Do I naturally socialize, or do I perform socializing?
What parts of connection feel good to me, and what parts feel confusing, exhausting, or high-pressure?
After social interaction, do I feel nourished, neutral, or like I need to lie face-down on the floor and become one with the carpet?
Executive function and daily life
What daily tasks repeatedly break down for me, even when I care deeply?
Do I struggle more with knowing what to do, starting what I know, or sustaining what I start?
What systems have helped me function—and how much do I rely on urgency, fear, or last-minute adrenaline?
Sensory and nervous system awareness
What sensory experiences consistently dysregulate me?
What environments make me feel safer, clearer, and more like myself?
Do I minimize my sensory needs because they seem “small,” even though they affect my whole day?
Masking and burnout
What do people assume is easy for me that is actually very effortful?
When do I feel most masked?
What happens to me when I can no longer maintain the mask?
Self-trust and next steps
If I believed my patterns were real, what would I stop blaming myself for?
What support would I ask for if I stopped trying to prove I was struggling “enough”?
What would change if I approached my brain with curiosity instead of suspicion?
Final reminder
If you are asking, “Do I have AuDHD?” there is a decent chance you are not asking because it is trendy.
You are asking because something in your life has not made sense in the shape it was handed to you.
And sometimes the beginning of healing is not a perfect answer.
Sometimes it is finally asking a better question.
Not:
What is wrong with me?
But:
What pattern has been here all along?
What has this brain been trying to manage?
What would compassion look like if I stopped using neurotypical ease as the measure of my worth?
Because whether you end up identifying as AuDHD or not, this part is still true:
A brain can be different without being defective.
A life can be hard without it being your fault.
And understanding yourself is not self-indulgence.
It is how you stop fighting your own wiring long enough to build a life that actually fits.