
“Is It ADHD… or Just Kid Stuff?”
A Science-Backed Guide for Parents Who Are Spiraling (Totally Understandably)

First: if you’ve Googled “does my child have ADHD” at 11:47pm while holding your breath… welcome. You’re not failing. You’re noticing patterns and trying to make sense of them. That’s parenting in 2026: equal parts love, logistics, and low-grade existential dread.
Also: I’m not your child’s clinician, so this isn’t a diagnosis. But I can walk you through what research and neuroscience actually say, what signs matter most, why diagnosis is tricky, and what you can do next—without panic-googling your way into the void.
What ADHD actually is (and what it isn’t)
ADHD is a neurodevelopmental condition—meaning it’s related to how the brain develops and regulates attention, impulse control, activity level, emotions, and executive function (planning, working memory, self-monitoring, etc.). Centers for Disease Control and Prevention describes it as a common neurodevelopmental disorder where children may struggle with attention, impulsivity, and/or hyperactivity.
ADHD is not:
a character flaw
“bad parenting”
laziness
a lack of discipline
“too much screen time” (screens can amplify symptoms, but they don’t magically create a neurodevelopmental disorder)
ADHD is:
a brain-based difference in self-regulation systems
often highly heritable (runs in families)
commonly paired with other things (anxiety, learning differences, sleep issues, autism, language delays—like a buy-one-get-several-free deal nobody asked for)
The neuroscience in plain language: why your child’s brain might “hit different”
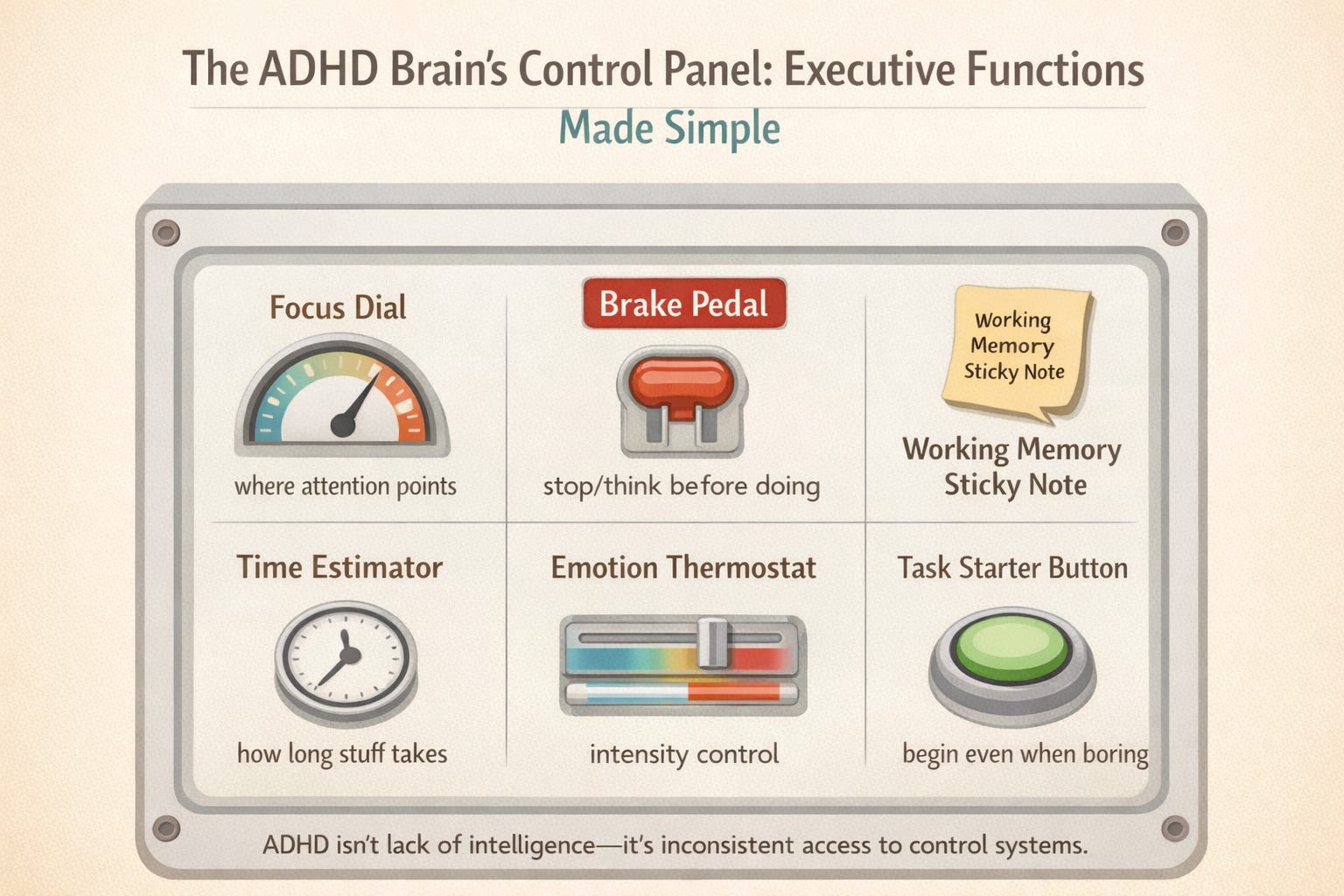
ADHD is strongly linked to differences in brain networks that manage attention and control, especially circuits involving the prefrontal cortex (the “air traffic control” of the brain) and its connections with deeper regions involved in movement, reward, and habit.
One of the most parent-relieving findings: many kids with ADHD show a delay in cortical maturation, especially in regions tied to attention and executive function. In a major brain-imaging study, cortical development patterns were similar, but lagged behind in ADHD.
That doesn’t mean “your child is behind” as a person. It means the timing and regulation of brain development can differ—so the demands of school/life may outpace the brain’s current scaffolding.
And yes, dopamine and norepinephrine systems (key for motivation, focus, and effort regulation) are part of the picture—especially in how the brain filters distractions and sustains goal-directed behavior.
Signs and symptoms: what to look for (beyond “they’re energetic”)
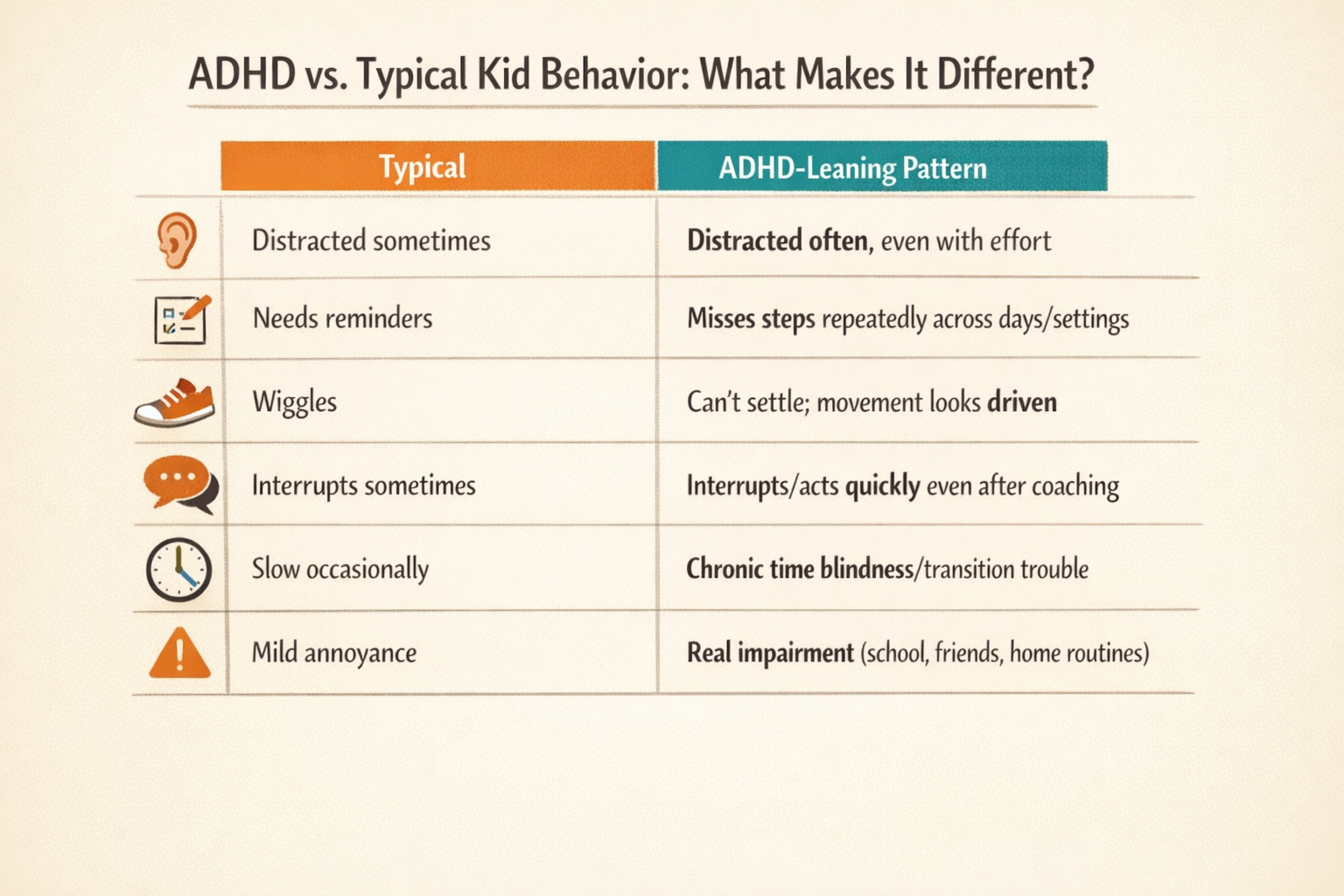
Here’s the big rule that clinicians use: it’s not just the behavior—it’s the pattern + the impact.
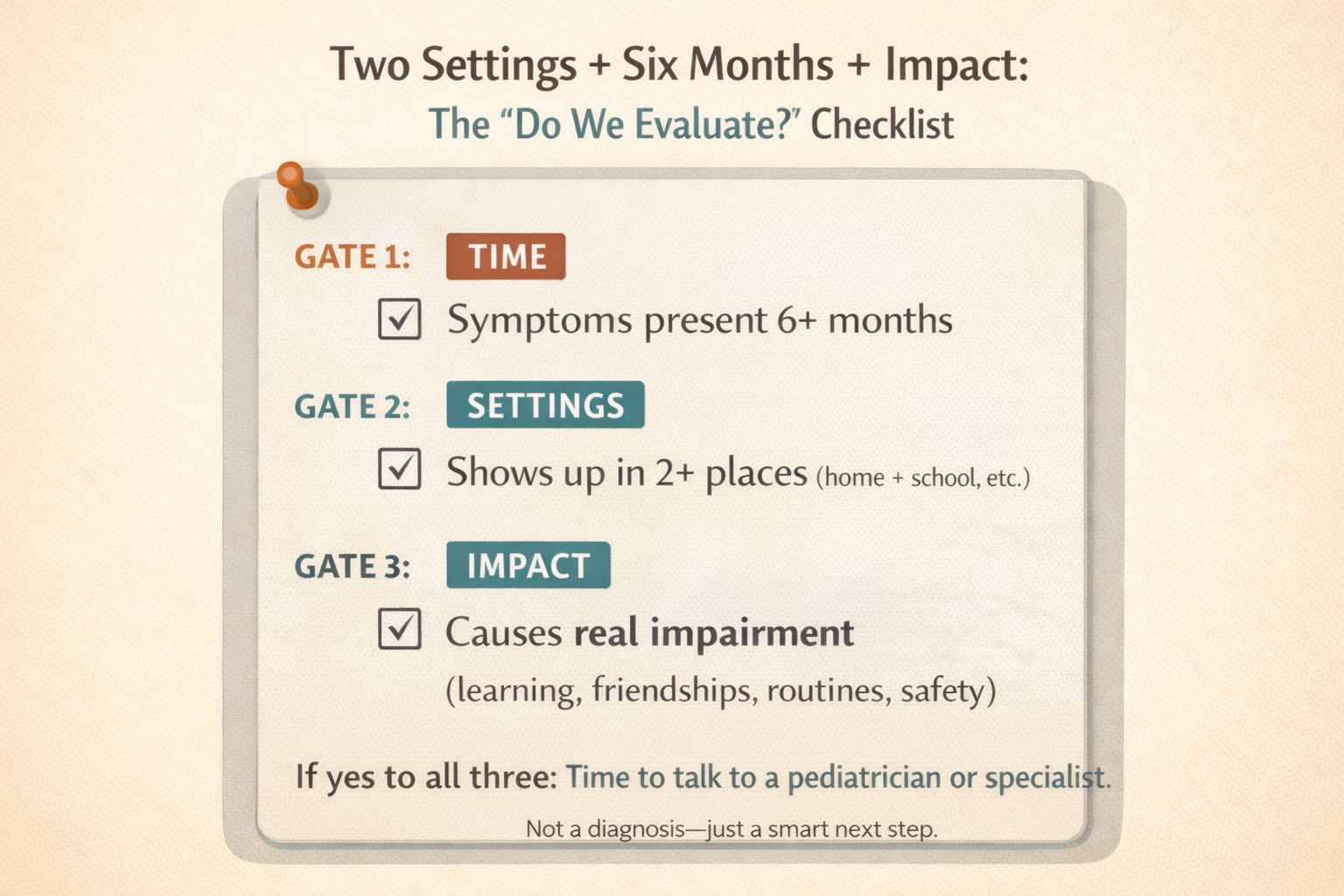
According to diagnostic standards, symptoms must:
last at least 6 months
show up in two or more settings (like home and school)
have started before age 12
cause real impairment in functioning (learning, relationships, daily life)
1) Inattention (often missed, especially in girls and “well-behaved” kids)
Common signs (especially when it’s more than developmental):
frequently loses track of steps (“I forgot what I was doing” energy all day)
struggles to start tasks and finish them (not just “doesn’t want to”)
seems not to listen (but it’s more like attention slips away)
forgetful in daily routines even with reminders
makes “careless” mistakes because details vanish under pressure
daydreamy, slow to shift gears, overwhelmed by multi-step directions
2) Hyperactivity (not always “bouncing off walls”)
Hyperactivity can look like:
constant movement, fidgeting, climbing when it’s not safe/expected
talks excessively
can’t stay seated when it’s required
looks “driven by a motor”
But it can also show up as internal restlessness, especially as kids get older.
3) Impulsivity (the “my brain hit SEND” category)
Signs include:
blurts out answers, interrupts, struggles to wait
big reactions with tiny pause between feeling → doing
risky choices, social misreads, “I didn’t think” moments
4) Emotional regulation (not always in the diagnostic headline, but VERY real)
Many kids with ADHD also struggle with:
fast frustration → meltdown
rejection sensitivity (“Nobody likes me!” after one neutral comment)
intense emotions that fade quickly but leave chaos behind
This matters because emotional dysregulation often drives the family stress more than the attention piece.
“But… aren’t these normal kid behaviors?” Yep. That’s why diagnosis is hard.
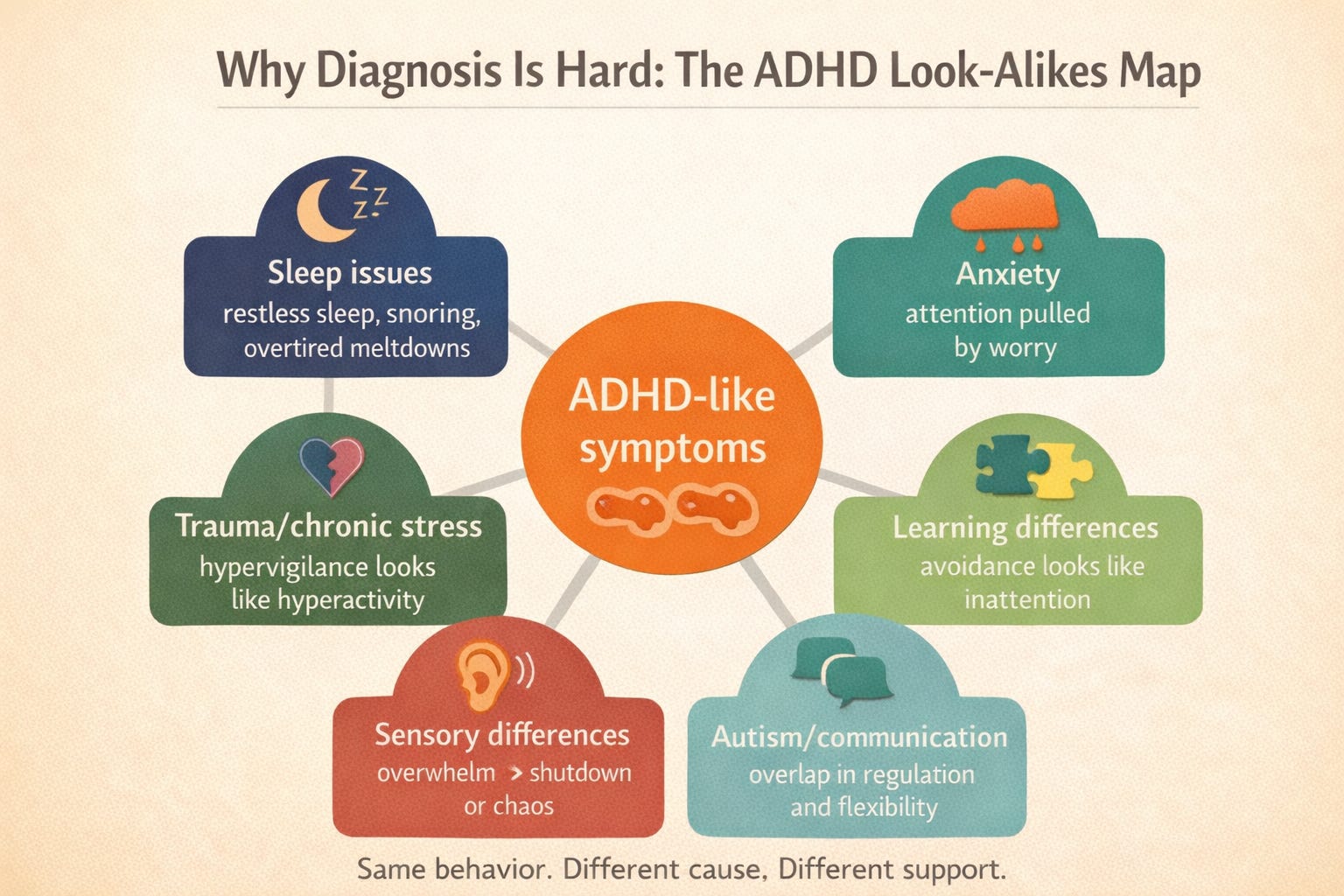
ADHD is difficult to diagnose because the symptoms overlap with normal development and with a bunch of other issues that can mimic ADHD.
Why it can look like ADHD (but isn’t)
National Institute of Mental Health notes that stress, sleep disorders, anxiety, depression, and other conditions can cause similar symptoms, and that a thorough evaluation is needed to sort out causes and effective treatments.
Common “ADHD look-alikes” include:
sleep problems (snoring, restless sleep, not enough sleep)
anxiety (inattention from worry)
trauma or chronic stress (hypervigilance can look like hyperactivity)
learning disorders (avoidance looks like “won’t focus”)
sensory processing differences
autism (overlapping executive function and regulation needs)
Why kids can look fine at school but fall apart at home (or vice versa)
Because attention is context-dependent. A child may hold it together where structure is high and expectations are clear—then completely unravel when the day ends and their nervous system finally unclenches.
Why clinicians need more than one perspective
Good evaluations include input from parents and teachers, plus rating scales and a developmental/medical history. The American Academy of Pediatrics guideline recommends initiating an evaluation for children ages 4–18 who show academic/behavioral problems with symptoms of inattention/hyperactivity/impulsivity.
And the truth bomb
There’s no brain scan that diagnoses ADHD in routine care. Diagnosis is still primarily clinical, based on patterns and impairment across settings.
Why seeking diagnosis can be a game-changer (even if you’re nervous about labels)
A diagnosis isn’t a life sentence. It’s a map.
It can unlock:
school supports (behavior plans, accommodations, 504/IEP pathways depending on need)
evidence-based therapy, especially parent training in behavior management for young kids
clarity around comorbidities (anxiety, learning issues, etc.)
better child self-understanding: “My brain needs different supports” instead of “I’m bad”
For preschoolers, experts recommend behavior therapy first, specifically parent training in behavior management—this is a big deal because it gives you tools that work with the brain you’ve got, not the brain you wish you had that day.
For older kids, treatment plans may include behavior therapy, school supports, and sometimes medication—based on severity and needs.
And here’s the poetic part: early support reduces the amount of shame a child has to carry.
Because untreated ADHD often gets mislabeled as “careless,” “defiant,” or “not trying”—and that can quietly erode self-worth.
When it’s time to get evaluated: a simple decision filter
Consider pursuing an evaluation if:
the pattern has lasted 6+ months
it shows up in more than one setting
it’s causing consistent problems (learning, friendships, family life, safety)
you’re using normal parenting tools and it’s still like trying to nail Jell-O to a wall
You can start with your pediatrician, a child psychologist, developmental-behavioral pediatrician, or a neuropsych evaluation depending on access and complexity.
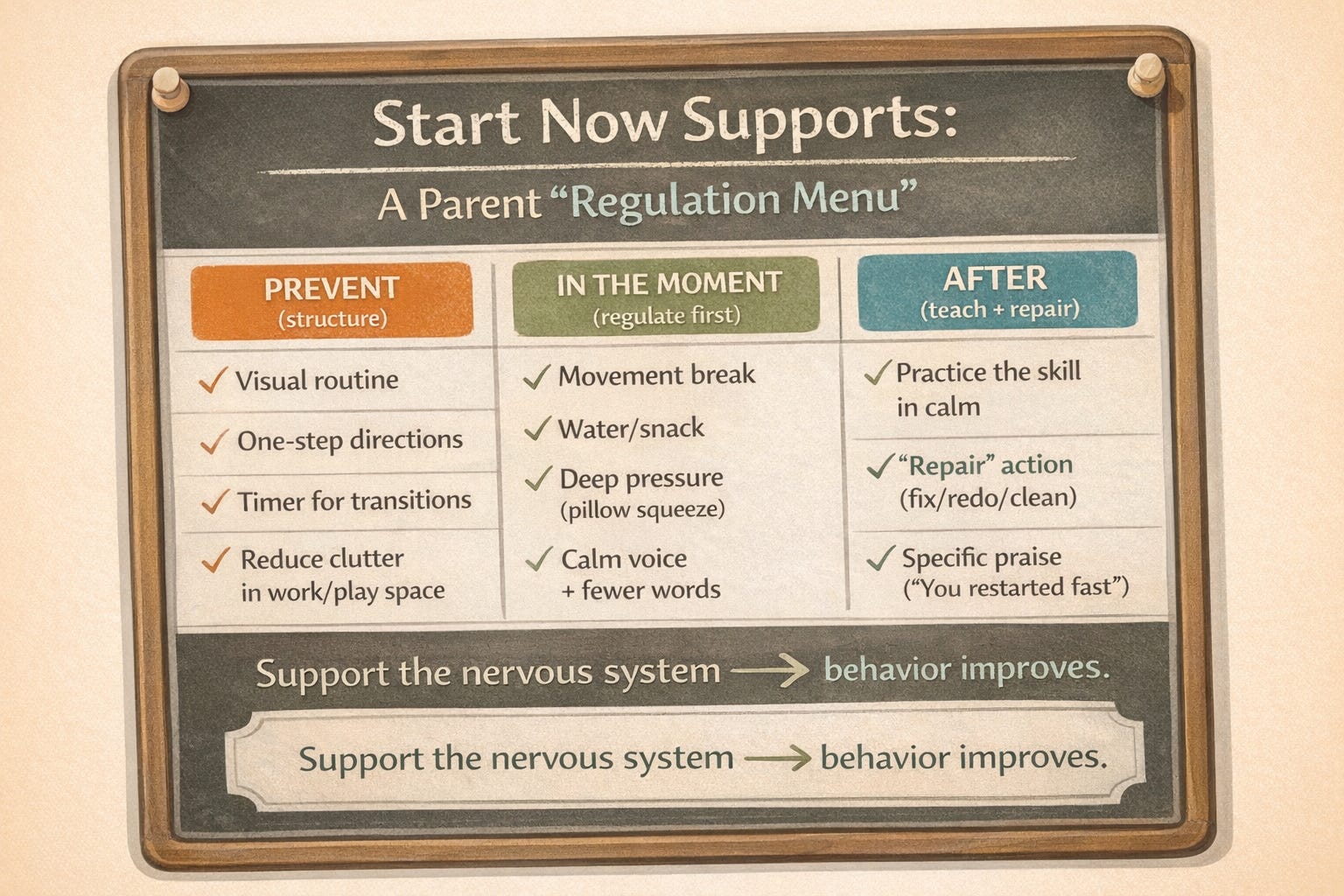
Practical strategies you can start now (whether or not you have a diagnosis yet)
These are ADHD-friendly supports that also help many kids in general—so you’re not “doing the wrong thing” if it turns out to be something else.
1) Externalize the brain
Visual routines (morning, bedtime, homework)
Checklists with pictures for younger kids
One-step directions, then the next step
Timers for transitions (“When it beeps, we move”)
2) Make instructions bite-sized
Instead of: “Clean your room.”
Try: “Put all the socks in the hamper. I’ll come back in 3 minutes.”
3) Build regulation before you demand behavior
If your child is dysregulated, logic is a decorative pillow.
Try:
movement breaks (jumping, animal walks)
deep pressure (squish pillow, weighted lap pad if appropriate)
snack + water (low blood sugar is chaos fuel)
4) Use consequences that teach, not punish
ADHD brains often struggle with delayed cause/effect.
Go for:
immediate feedback
“repair” actions (fix it, clean it, redo it)
praise that’s specific: “You started right away—nice job shifting gears.”
5) Collaborate with school like it’s a team sport
Ask for:
seating that reduces distraction
movement opportunities
chunked assignments
repeated directions in writing/pictures
a daily home-school check-in if needed
6) Track patterns like a calm scientist
For 2 weeks, jot:
sleep
food
screen time
big transitions
meltdowns (time + trigger)
This helps clinicians and helps you see what’s really driving the hard moments.
Reflection journal prompts (for the parent brain that needs a flashlight, not a courtroom)
Use these to reduce panic and increase clarity:
Pattern spotting
When does my child seem most regulated (time of day, setting, activity)?
When do things fall apart most often—and what happens right before?
Demand vs. skills
What expectations might be outpacing my child’s current skills (attention, transitions, emotional control)?
If I assumed this was a skill gap, what support would I add instead of what punishment would I give?
Environment scan
Where is distraction highest? Noise? Visual clutter? Too many instructions?
What’s one tiny environmental change that could make things 10% easier?
Nervous system check
What does my child’s “early warning sign” look like before a meltdown?
What helps them come back fastest: movement, connection, quiet, pressure, humor, snack?
Parent compassion
What story am I telling myself about this (“I’m failing,” “They’re doing it on purpose”)?
What’s a more accurate story that still holds everyone accountable?
If you take one thing from this
ADHD isn’t a moral issue. It’s a regulation issue.
If you’re seeing consistent patterns that affect your child’s learning, relationships, or daily functioning, seeking an evaluation is a responsible next step, not an overreaction.
If you tell me your child’s age and the top 3 struggles you’re seeing (home/school/social), I’ll tailor a “what to document” list + a starting strategy plan that fits your real life (not an imaginary life where everyone has endless patience and matching socks).