
Medication Is Not a Moral Failure: The AuDHD Guide to Brain Chemistry Without the Shame Spiral
Stimulants, Non-Stimulants, Mood Meds, Anxiety Meds, and Why Your Brain Is Not “Lazy”—It’s Running Windows 97 With 46 Tabs Open

Disclaimer before we get spicy:
I am not a doctor, psychiatrist, pharmacist, or tiny wizard living inside your pill bottle. This post is for education and reflection only. Medication decisions should always be made with a qualified healthcare provider who knows your body, history, diagnoses, other medications, side effects, risks, and the general haunted mansion that is your nervous system.
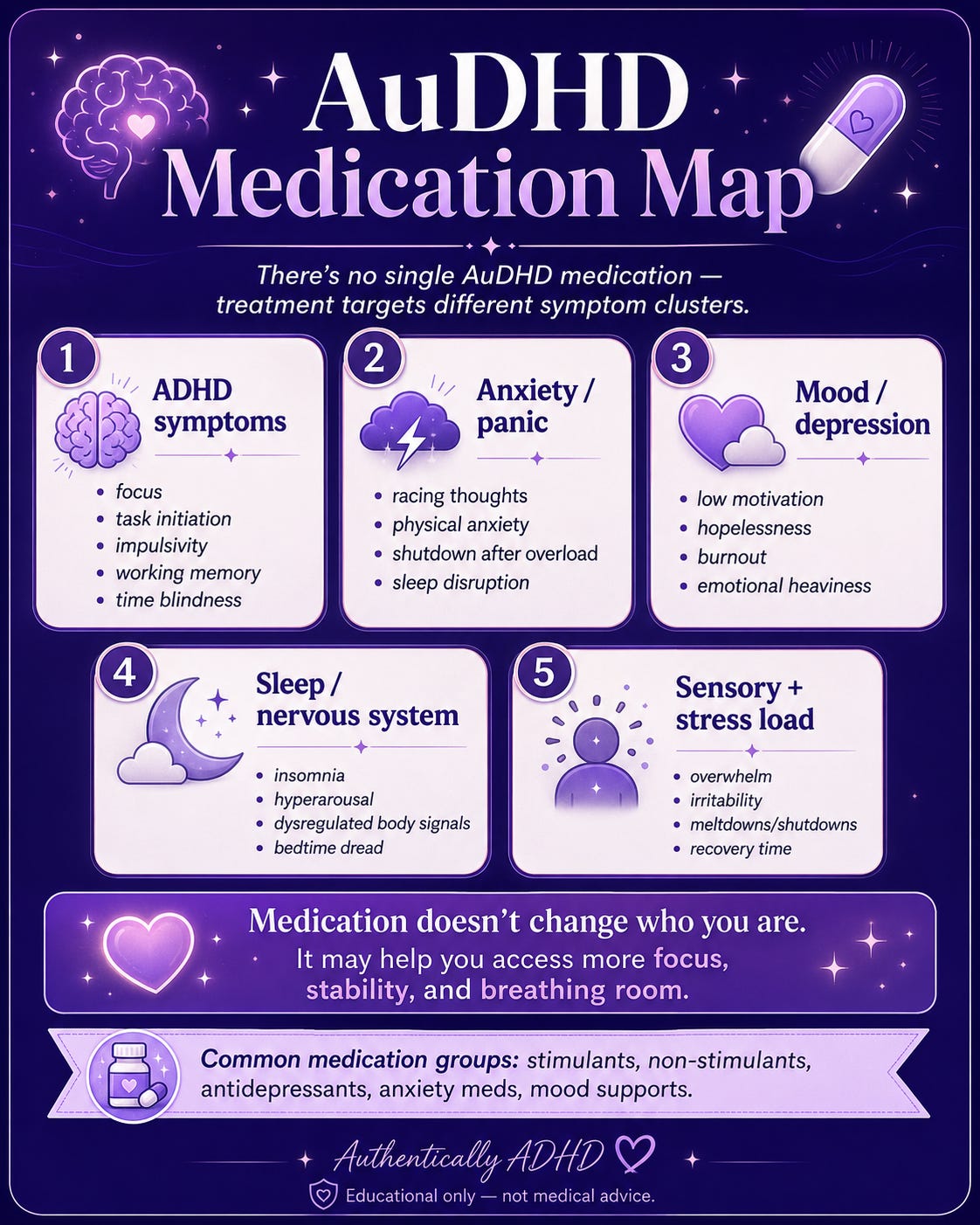
Also: there is no one-size-fits-all AuDHD medication. There is no magic pill that makes autism go away, because autism is not a cold sore. Medication can help target specific symptoms or co-occurring conditions like ADHD, anxiety, depression, sleep issues, panic, irritability, mood instability, chronic pain, or emotional dysregulation. But it does not erase your neurotype. It may, however, help turn the brain-volume knob down from “fork in garbage disposal” to “still weird, but functional.”
And honestly? We love that for us.
First, What Are We Actually Treating?
AuDHD is the co-occurrence of autism and ADHD. Cute little acronym. Absolute neurological group project from hell.
ADHD often brings challenges with attention regulation, impulsivity, task initiation, working memory, time awareness, emotional regulation, and motivation. Autism can bring differences in sensory processing, communication, predictability needs, social energy, monotropism, nervous system intensity, transitions, and burnout.
Together, they can create a brain that says:
“I need routine.”
“Routine is boring.”
“I need stimulation.”
“Too much stimulation is a war crime.”
“I want connection.”
“Please do not perceive me.”
“I need to start the task.”
“Actually, I will stare at the task until we both die.”
Medication does not “fix” AuDHD. That language can exit through the gift shop. Medication may support specific brain systems so the person has more access to their own tools.
Think of it less like “curing the brain” and more like giving the brain better Wi-Fi, fewer pop-up ads, and maybe a security team for the emotional raccoons.
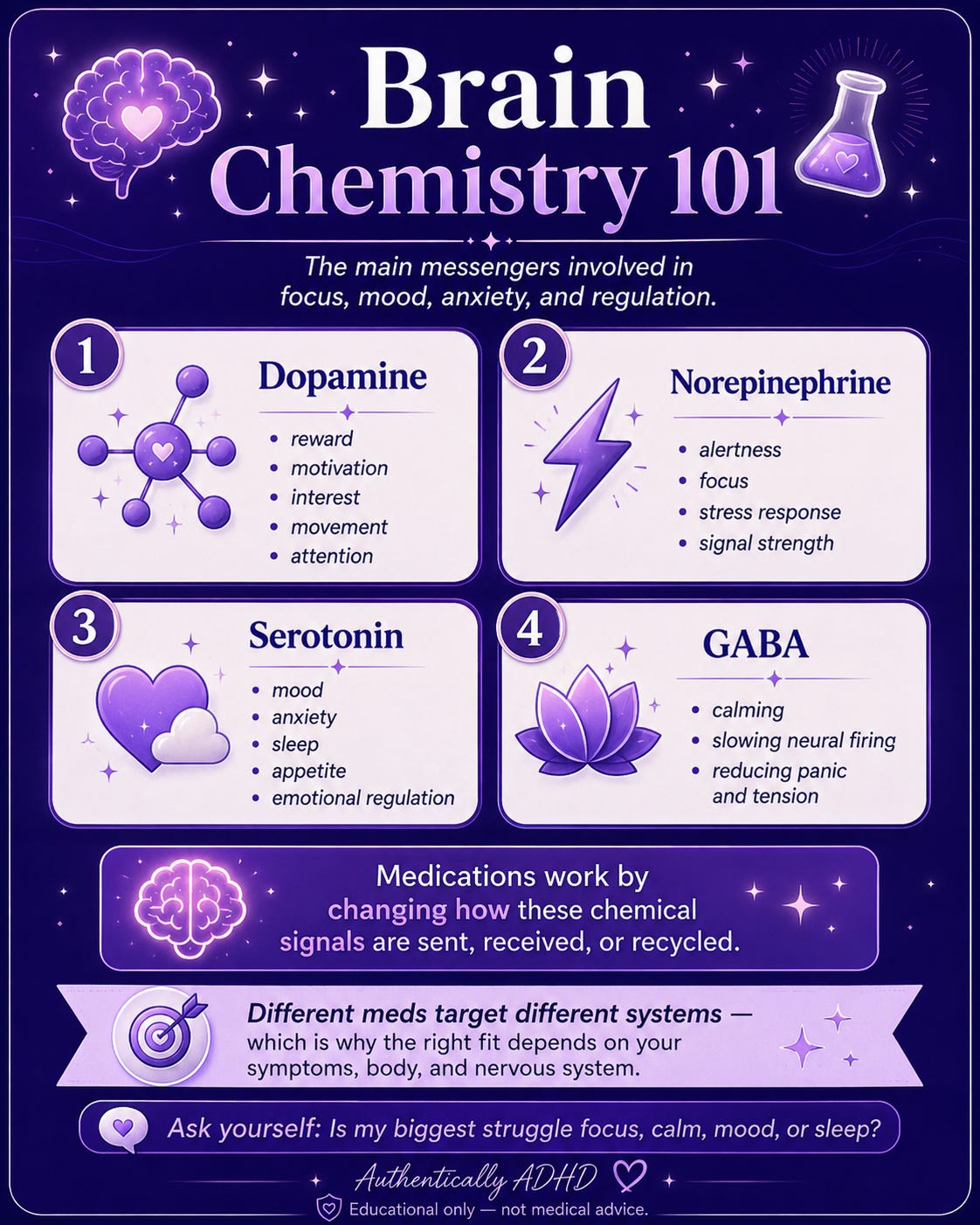
The Brain Chemistry Basics: Dopamine, Norepinephrine, Serotonin, and GABA
Before we talk meds, let’s talk neurotransmitters—the brain’s tiny chemical text messages.
Dopamine is involved in reward, motivation, learning, movement, attention, and “will I do the thing or will I become furniture?” ADHD is not simply “low dopamine,” but dopamine pathways are part of attention, motivation, and reward regulation.
Norepinephrine helps with alertness, focus, stress response, vigilance, and signal amplification. Too little can feel like fog. Too much can feel like being hunted by an email.
Serotonin is involved in mood, anxiety, sleep, appetite, pain, and emotional regulation. It is not just the “happy chemical,” despite what inspirational mugs would like us to believe.
GABA is the brain’s main calming/inhibitory neurotransmitter. It helps slow neural firing. It is basically the nervous system’s weighted blanket, except sometimes the blanket is missing, damp, or being used by a raccoon.
Different medications target different systems. Some help increase access to dopamine and norepinephrine. Some calm the stress response. Some support mood and anxiety pathways. Some help sleep. Some are used off-label because brains did not read the brochure.
1. Stimulants: The “Turn the Executive Function Lights On” Meds
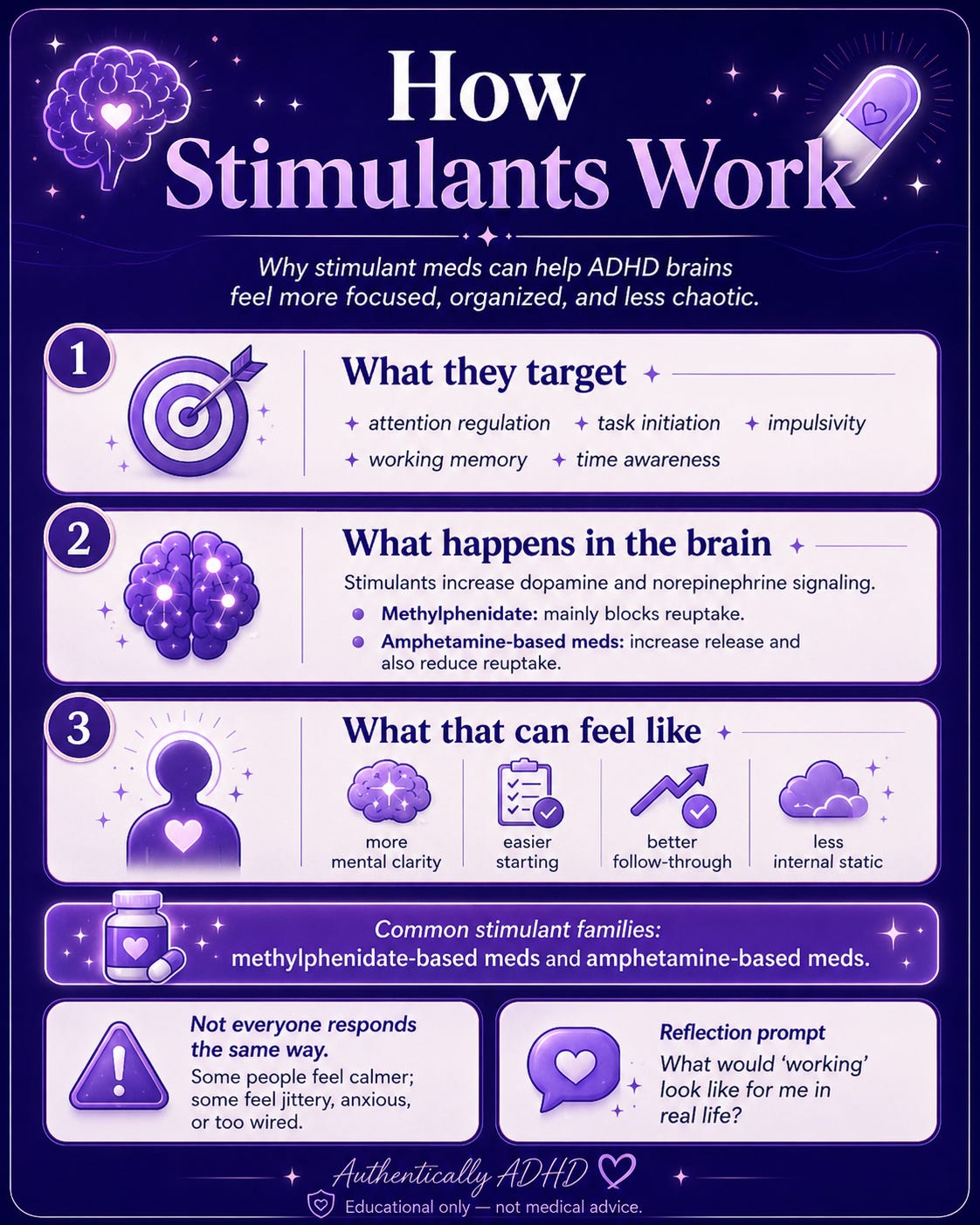
Stimulants are often first-line medications for ADHD. They are called stimulants because they stimulate the central nervous system, which sounds like something that should make ADHD worse, but brains are rude and science is weird.
For many ADHD brains, stimulants can actually help reduce internal chaos. Instead of creating “more energy,” they may help the brain regulate attention, impulse control, and task initiation.
Basically, the brain stops acting like every thought is trying to crowd-surf at the same concert.
Common stimulant families
Methylphenidate-based medications
Examples may include Ritalin, Concerta, Metadate, Focalin/dexmethylphenidate, and related formulations.
Methylphenidate medications primarily work by increasing dopamine and norepinephrine signaling, especially by blocking the transporters that normally vacuum those neurotransmitters back up. More availability in the synapse can mean better signal strength in brain circuits involved in attention, inhibition, and executive function.
Translation: the brain’s “do the thing” committee may finally show up to the meeting.
Amphetamine-based medications
Examples may include Adderall, Dexedrine, Vyvanse/lisdexamfetamine, and related formulations.
Amphetamines also increase dopamine and norepinephrine activity. They can block reuptake and increase release of these neurotransmitters into the space between neurons. Vyvanse is a prodrug, meaning the body converts it into its active form over time, which can create a smoother effect for some people.
Translation: instead of screaming “FOCUS!” at yourself like a motivational goblin, the medication may help your attention system have actual fuel.
What stimulants may help with
For some AuDHDers, stimulants may help with:
task initiation
focus and sustained attention
impulsivity
emotional reactivity
working memory
time awareness
mental fatigue
binge-scrolling paralysis
the “I know what to do but my body has filed a formal complaint” problem
But stimulants are not fairy dust. Some people feel calmer. Some feel more focused. Some feel like they have accidentally swallowed a corporate productivity seminar. Some feel anxious, flat, irritable, sweaty, hungry never, or tired in a way that makes no sense.
Brains are not vending machines. You do not always press “dopamine” and receive “functional adult.”
Stimulants and AuDHD: The Sensory Plot Twist
For AuDHD folks, stimulants can be amazing, complicated, or both. Sometimes focus improves but sensory sensitivity becomes louder. Sometimes task initiation improves but appetite disappears into the witness protection program. Sometimes the medication works beautifully until it wears off, and then the brain enters its “Victorian ghost child in a hallway” era.
Possible experiences can include:
appetite suppression
insomnia or sleep disruption
increased heart rate or blood pressure
anxiety or jitteriness
jaw clenching
dry mouth
irritability
emotional crash as it wears off
sensory sensitivity feeling sharper
feeling “too quiet” or unlike yourself
rebound symptoms later in the day
This does not mean stimulants are bad. It means they are powerful tools, not personality seasoning.
Active Processing Question
When I imagine medication “working,” what am I hoping it changes: focus, task initiation, emotional reactivity, sensory overwhelm, fatigue, anxiety, impulsivity, or something else?
Because “I just want to function” is valid, but your provider needs a more specific target than “please remove the bees from my skull.”
2. Non-Stimulants: The Slow-Burn Support Team
Non-stimulants are ADHD medications that do not work like classic stimulants. They may be used when stimulants are not tolerated, are not effective enough, worsen anxiety/sleep/appetite, interact with other health needs, or are not the best fit for a person’s nervous system.
They usually do not kick in as quickly as stimulants. Stimulants can sometimes be felt the same day. Non-stimulants often need time to build effect. They are less “light switch” and more “crockpot with paperwork.”
Atomoxetine
Atomoxetine, often known by the brand name Strattera, is a selective norepinephrine reuptake inhibitor. It increases norepinephrine availability by blocking the norepinephrine transporter.
Norepinephrine matters for alertness, attention, and executive function. Atomoxetine may be helpful for ADHD symptoms, especially when stimulant side effects are rough or when anxiety, substance misuse risk, or sleep issues complicate the picture.
It is not usually a “take it and suddenly clean your entire house while crying to a podcast” medication. It is slower and steadier.
Possible side effects may include stomach upset, appetite changes, sleepiness or insomnia, dry mouth, mood changes, and changes in heart rate or blood pressure. Some people love it. Some people feel nothing. Some people feel like their stomach has opened a complaint department.
Viloxazine ER
Viloxazine ER, known by the brand name Qelbree, is another non-stimulant ADHD medication. Its exact mechanism in ADHD is not fully understood, but it is thought to involve norepinephrine reuptake inhibition and may also influence serotonin systems.
For some people, this may help attention, impulsivity, and emotional regulation. Like atomoxetine, it is not a stimulant and may take time.
Possible side effects may include sleepiness, fatigue, appetite changes, nausea, irritability, or insomnia. The nervous system loves irony. A medication may cause sleepiness in one person and insomnia in another because apparently consistency was not in the budget.
Guanfacine and Clonidine
Guanfacine and clonidine are alpha-2 adrenergic agonists. They are not stimulants. They work partly by affecting norepinephrine-related signaling and reducing sympathetic nervous system output.
Guanfacine is more selective for alpha-2A receptors, which are especially relevant to prefrontal cortex functioning. The prefrontal cortex is involved in attention, impulse control, emotional regulation, planning, and the sacred art of not interrupting someone even though your thought is on fire.
Clonidine also stimulates alpha-2 receptors in the brain and can reduce sympathetic outflow. It is often thought of as more calming/sedating for many people.
These medications may be used for hyperactivity, impulsivity, emotional reactivity, sleep issues, tics, aggression/rage patterns, or nervous system overactivation, depending on the person and prescriber.
For some AuDHDers, alpha-2 agonists are less about “focus laser” and more about “can my nervous system stop acting like a smoke alarm with abandonment issues?”
Possible side effects may include sleepiness, dizziness, low blood pressure, fatigue, dry mouth, constipation, or feeling slowed down. These meds can affect blood pressure and should not be started, stopped, or changed without medical guidance.

Active Processing Question
Is my biggest daily struggle more like “I cannot start,” “I cannot stop,” “I cannot calm down,” “I cannot stay awake,” or “I cannot tolerate the sensory crime scene of being alive”?
Different medication classes aim at different parts of the chaos.
3. Bupropion: The Off-Label Dopamine/Norepinephrine Cousin
Bupropion, often known as Wellbutrin, is an antidepressant that is sometimes used off-label for ADHD, especially when depression and ADHD symptoms overlap.
It is often described as a norepinephrine-dopamine reuptake inhibitor. It does not work like SSRIs because it is not primarily serotonergic. For some people, it may support motivation, energy, mood, and attention.
This can be especially relevant when the person’s depression looks like:
no motivation
low energy
task paralysis
“I have become a decorative throw pillow”
difficulty feeling reward
brain fog
emotional flatness
However, bupropion can be activating. For some people, that is helpful. For others, it can increase anxiety, irritability, insomnia, or make the nervous system feel like it drank cold brew through a fire hose.
It may also not be appropriate for people with certain seizure risks or eating disorder histories, so this is very much a prescriber conversation.
Active Processing Question
When I say “depressed,” do I mean sad, numb, exhausted, hopeless, understimulated, burned out, ashamed, physically depleted, or unable to access reward?
Those are not all the same beast. Some are dragons. Some are possums in a hoodie.
4. SSRIs: Anxiety and Depression Support, Not ADHD Meds
SSRIs—selective serotonin reuptake inhibitors—are commonly prescribed for depression, anxiety disorders, OCD, panic, PTSD symptoms, and related mood/anxiety patterns.
Examples may include sertraline, fluoxetine, escitalopram, citalopram, paroxetine, and others.
SSRIs work by inhibiting the reuptake of serotonin, leaving more serotonin available in the synaptic space over time. The downstream effects are more complicated than “more serotonin equals happy,” because the brain is not a glitter jar. But serotonin signaling is involved in mood regulation, anxiety, sleep, appetite, and emotional processing.
For AuDHDers, SSRIs may help when anxiety or depression is its own full-time goblin. They may reduce panic, rumination, obsessive loops, rejection sensitivity spirals, or the feeling that one mildly awkward conversation means you must move to a new state and become a mushroom farmer.
But SSRIs do not directly treat ADHD executive dysfunction. If your main issue is task initiation, working memory, or dopamine-based motivation, an SSRI might help the emotional weather but not necessarily build the bridge to Doing The Thing.
Possible side effects may include nausea, sleep changes, emotional blunting, sexual side effects, sweating, headaches, appetite changes, or activation early on. Some people feel steadier. Some feel flat. Some feel like their anxiety packed a smaller suitcase but still came on the trip.
Active Processing Question
Is anxiety the main barrier, or is anxiety happening because my ADHD/autistic needs are unsupported?
Because sometimes the “anxiety disorder” is actually a nervous system screaming, “We have ignored sensory needs, sleep, transitions, hunger, and boundaries for 14 years, Susan.”
5. SNRIs: Mood, Anxiety, Pain, and the Norepinephrine Lever
SNRIs—serotonin-norepinephrine reuptake inhibitors—include medications like venlafaxine, desvenlafaxine, and duloxetine.
They work by increasing serotonin and norepinephrine signaling. Because norepinephrine is involved in alertness, attention, and stress response, SNRIs can feel different from SSRIs. Some people find them more energizing. Some find them helpful for depression with fatigue or chronic pain. Some find them too activating.
Duloxetine is also commonly used for certain pain conditions, which matters because a lot of neurodivergent people live in bodies that act like they were assembled by a committee during a thunderstorm.
SNRIs may be prescribed for:
depression
generalized anxiety
panic symptoms
chronic pain
nerve pain
fatigue-heavy mood symptoms
emotional dysregulation related to mood/anxiety
Possible side effects may include nausea, sweating, blood pressure changes, insomnia, sleepiness, dry mouth, sexual side effects, and discontinuation symptoms if stopped suddenly.
SNRIs can be powerful. They are not “just antidepressants.” They affect multiple neurotransmitter systems, which means they deserve respect, monitoring, and absolutely not a casual “oops I forgot for four days” relationship if your body is sensitive.
Active Processing Question
Do I notice mood symptoms in my thoughts, my body, my energy, my pain levels, my sleep, or my ability to care about anything?
Mood is not only sadness. Sometimes it is a body made of wet cement and a brain playing dial-up noises.
6. Tricyclic Antidepressants: Old-School, Strong, and Not Here to Be Cute
Tricyclic antidepressants, or TCAs, are an older class of antidepressants. Examples include amitriptyline, nortriptyline, imipramine, and others.
TCAs can affect serotonin and norepinephrine by blocking their reuptake. They also interact with other receptor systems, including histamine and acetylcholine receptors, which is part of why they can be sedating and why side effects can be… let’s call them “vintage.”
Amitriptyline, for example, is sometimes used for depression, migraine prevention, nerve pain, sleep, and certain chronic pain conditions. It can be sedating, which may be helpful for some people and absolutely not helpful for others who already wake up feeling like they were resurrected incorrectly.
Possible side effects may include:
dry mouth
constipation
sleepiness
weight changes
dizziness
blurred vision
urinary retention
heart rhythm concerns in some people
grogginess
“my mouth is the Sahara and my thoughts are soup”
TCAs can also interact with other meds and can be dangerous in overdose, so they require careful prescribing and monitoring.
For some AuDHDers, a TCA may be part of the plan when sleep, pain, migraine, anxiety, or mood are tangled together like headphones in a junk drawer. Again: not an autism med. Not an ADHD first-line med. But sometimes part of the whole-person picture.
Active Processing Question
Is my nervous system struggling mostly during the day, at night, during transitions, during social recovery, during pain flares, or during emotional comedowns?
The timing of symptoms matters. The brain leaves clues. Annoying little breadcrumbs, but breadcrumbs.
7. Anxiety Medications: When the Alarm System Won’t Shut Up
Anxiety in AuDHD can come from many places:
sensory overload
unpredictability
trauma
masking
social confusion
executive dysfunction
panic disorder
OCD
burnout
interoception differences
being alive in capitalism, which frankly should come with a complimentary weighted blanket
Medication for anxiety depends on the type of anxiety and the person’s history.
Benzodiazepines
Examples include clonazepam, lorazepam, alprazolam, and diazepam.
Benzodiazepines enhance the effect of GABA, the brain’s major inhibitory/calming neurotransmitter. They can reduce acute anxiety, panic, muscle tension, and nervous system overactivation.
They can also cause sedation, memory issues, coordination problems, tolerance, dependence, withdrawal risks, and dangerous interactions with alcohol, opioids, or other sedating medications.
So yes, they can be useful. Also yes, they are not emotional Skittles.
For AuDHDers with panic, severe anxiety, or sleep-related nervous system activation, benzodiazepines may be prescribed carefully. But long-term use requires serious conversation with a provider because dependence and withdrawal are not side quests you want to unlock accidentally.
Buspirone
Buspirone is a non-benzodiazepine anxiety medication sometimes used for generalized anxiety. It works through serotonin receptor activity, especially 5-HT1A partial agonism. It is not fast-acting like benzodiazepines and typically takes time.
It is not usually sedating in the same way, and it does not carry the same dependence risk as benzodiazepines. But it also may not help acute panic in the moment.
It is very much a “background anxiety volume” medication, not a “my nervous system is on fire right now” fire extinguisher.
Active Processing Question
Is my anxiety a sudden panic spike, a constant hum, a trauma response, a sensory overload signal, a social recovery cost, or a demand-avoidance alarm?
Because treating every anxiety signal the same is like using a fire extinguisher on a low phone battery. Dramatic, but not useful.
8. Mood Stabilizers and Antipsychotics: When Safety, Mood, or Irritability Are Bigger Players
Some AuDHDers are also diagnosed with bipolar disorder, major depression, PTSD, PMDD, OCD, severe anxiety, or other mood disorders. Some experience severe irritability, aggression, self-injury, panic, shutdowns, meltdowns, or mood instability that needs more support than ADHD meds alone.
This is where providers may consider medications like mood stabilizers or atypical antipsychotics.
Mood stabilizers
Examples may include lamotrigine, lithium, valproate/divalproex, carbamazepine, and others depending on diagnosis.
These are not ADHD medications. They are used for mood disorders, bipolar disorder, seizure disorders, or mood instability depending on the medication.
Lamotrigine, for example, is often discussed in mood contexts because of its role in bipolar depression maintenance, though its precise mechanism is complex and not fully reduced to one cute neurotransmitter explanation. Many mood stabilizers affect glutamate, sodium channels, GABA systems, intracellular signaling, or broader excitability patterns.
Translation: less “focus please” and more “can the mood volcano stop threatening the village?”
These meds can require monitoring and careful titration. Some have serious risks, like rash with lamotrigine or blood-level monitoring with lithium. These are absolutely not DIY meds. The vibes are not casual.
Atypical antipsychotics
Examples may include aripiprazole, risperidone, quetiapine, olanzapine, and others.
These medications affect dopamine and serotonin receptors in different ways. They may be prescribed for bipolar disorder, psychosis, severe depression augmentation, severe irritability, aggression, sleep, or agitation depending on the person and situation.
In autism, risperidone and aripiprazole are known for use in severe irritability/aggression in children and adolescents. That does not mean they treat “autism itself.” It means they may target dangerous or severe symptoms that can occur alongside autism.
Possible side effects can include weight gain, metabolic changes, sleepiness, movement symptoms, hormonal changes, restlessness, and more. These medications can be life-changing for some people and too heavy for others. Both things can be true.
Active Processing Question
Are my hardest symptoms about attention, anxiety, depression, sleep, sensory overload, trauma, rage, panic, or mood cycling?
Medication conversations get safer and more useful when we name the target instead of throwing a pharmaceutical dart at “I feel bad.”
Medication and AuDHD: Why Side Effects Can Feel So Personal
AuDHD nervous systems can be extra sensitive to internal changes. Interoception differences may make it hard to identify what is happening in the body until the body is basically holding a press conference.
A side effect may show up as:
“I feel weird but cannot explain how”
sudden rage
sensory intolerance
nausea
appetite disappearing
sleep getting weird
feeling emotionally flat
panic spikes
more shutdowns
more meltdowns
more social withdrawal
“my skin is too loud”
“my thoughts are wearing wet jeans”
This is why tracking can be so helpful. Not obsessive tracking. Not “create a spreadsheet so intense it needs its own therapist.” Just enough notes to notice patterns.
Helpful things to track:
sleep
appetite
anxiety
mood
focus
task initiation
irritability
sensory sensitivity
heart rate/blood pressure if advised
headaches
GI symptoms
medication timing
caffeine
menstrual cycle/hormonal changes
crashes or rebounds
“did I eat actual food or just vibes and a granola bar?”
Active Processing Question
What are my top three “this med might be helping” signs, and my top three “this med might not be a fit” signs?
Because when you are in the middle of a medication trial, memory becomes soup and vibes become evidence. Write it down. Future you deserves receipts.
The Shame Piece: Medication Does Not Mean You Failed
A lot of AuDHDers carry medication shame.
Maybe someone told you meds are a crutch.
Cool. Glasses are also a crutch. So are calendars, insulin, inhalers, noise-canceling headphones, and the emotional support water bottle you carry from room to room like a Victorian child with consumption.
Support is not cheating.
Medication does not make you less authentic. It does not make your needs fake. It does not mean you are broken. It means your brain-body system may benefit from chemical support, just like it may benefit from rest, accommodations, therapy, protein, movement, sensory tools, boundaries, and not forcing yourself to be a neurotypical productivity Roomba.
Also, not taking medication is valid. Taking medication is valid. Changing medication is valid. Needing multiple supports is valid. Having side effects is valid. Being scared is valid. Being hopeful is valid. Being angry that no one helped you sooner is extremely valid and frankly deserves its own dramatic soundtrack.
So How Do You Talk to a Provider Without Freezing?
Bring specifics. Providers cannot read your mind, and unfortunately “my brain is bees” is not yet a billing code.
Try naming:
What symptoms are most impairing?
When do they happen?
What have you already tried?
What helps even a little?
What makes it worse?
What are your biggest concerns?
Do you have sleep issues?
Do you have panic, depression, trauma, mood swings, or chronic pain?
Do you have a history of medication sensitivity?
Do you take supplements, cannabis, caffeine, or other meds?
What side effects would be a deal-breaker?
You are allowed to ask:
What symptom is this medication targeting?
How does it work?
How long before we know if it helps?
What side effects should I watch for?
What side effects are urgent?
What should I avoid combining it with?
What happens if I miss a dose?
How do we stop it safely if needed?
What are the alternatives?
That is not being difficult. That is informed consent wearing boots.

Final Thoughts: You Are Not a Bad Person for Needing Chemistry
AuDHD is not a character flaw. It is not laziness. It is not “not trying hard enough.” It is not a lack of planners, discipline, or inspirational beige morning routines.
It is a neurodevelopmental reality with real nervous system consequences.
Medication may not be the whole answer, but for some people, it is a door. A bridge. A dimmer switch. A little less static. A little more choice.
And choice matters.
Because the goal is not to become less autistic.
The goal is not to become less ADHD.
The goal is not to become a productivity machine with excellent email etiquette and no sensory needs.
The goal is access.
Access to your attention.
Access to your rest.
Access to your relationships.
Access to your body cues.
Access to your creativity.
Access to your actual self underneath the coping, masking, shame, burnout, and “why am I like this?” spiral.
You are not weak for needing support.
You are a nervous system trying to survive a world that often confuses “unsupported” with “unmotivated.”
And babe, that is not a medication problem.
That is a whole damn society problem.
But while we work on that?
You still deserve help.
You still deserve options.
You still deserve a brain that is not constantly trying to eat itself in the parking lot of Target.
And if medication is part of that support system, that does not make you less you.
It might just give you enough room to finally meet yourself without the static.
Free Medication Tracker Resource:
Download:
Simple Medication Tracker
Medication name: ___________________________
Dose: ___________________________
Start date: ___________________________
Prescriber: ___________________________
Why I’m taking it / target symptoms:
Daily Check-In
Date: ___________________
Day #: _______
Medication Timing
Time taken: ___________
With food? ☐ Yes ☐ No
Other meds/supplements taken today:
Quick Rating Scale
Rate each from 0–5
0 = none / not an issue
5 = intense / very noticeable
Focus / attention: _____ (0 1 2 3 4 5)
Task initiation: _____ (0 1 2 3 4 5)
Anxiety: _____ (0 1 2 3 4 5)
Mood: _____ (0 1 2 3 4 5)
Irritability: _____ (0 1 2 3 4 5)
Sensory sensitivity: _____ (0 1 2 3 4 5)
Energy level: _____ (0 1 2 3 4 5)
Appetite: _____ (0 1 2 3 4 5)
Sleep quality: _____ (0 1 2 3 4 5)
Body Side Effects
Check anything you noticed today:
☐ Nausea
☐ Headache
☐ Dry mouth
☐ Dizziness
☐ Racing heart
☐ Sleepiness
☐ Insomnia
☐ Appetite changes
☐ Stomach issues
☐ Sweating
☐ Jaw clenching
☐ Emotional flatness
☐ Rebound/crash
☐ Other: ___________________________
What I Noticed Today
What seemed better?
What seemed worse?
Anything weird, intense, or “my nervous system is auditioning for a horror film”?
End-of-Day Reflection
Overall, today felt:
☐ Better than usual
☐ About the same
☐ Worse than usual
☐ Mixed / confusing / brain soup
One thing I want to remember for my prescriber:
Weekly Pattern Check
At the end of the week, look back and answer:
Did the medication help the symptom it was supposed to target?
☐ Yes
☐ No
☐ Maybe
☐ Too soon to tell
Most noticeable benefit:
Most noticeable side effect:
Questions for my prescriber:
Do I want to keep tracking this another week?
☐ Yes
☐ No
☐ I need to talk to my prescriber first
Reminder: This tracker is for noticing patterns, not diagnosing yourself at 11:47 PM while spiraling on Google like a goblin with Wi-Fi. Always talk to your prescriber before changing, stopping, increasing, or mixing medications.