
Your Brain Isn’t “Just Sensitive”: The AuDHD Sound Map for Hyperacusis& Misophonia
Auditory Processing Disorders

People love to toss “sound sensitivity” into one messy bucket, like it’s all the same vibe.
Surprise. It’s not.
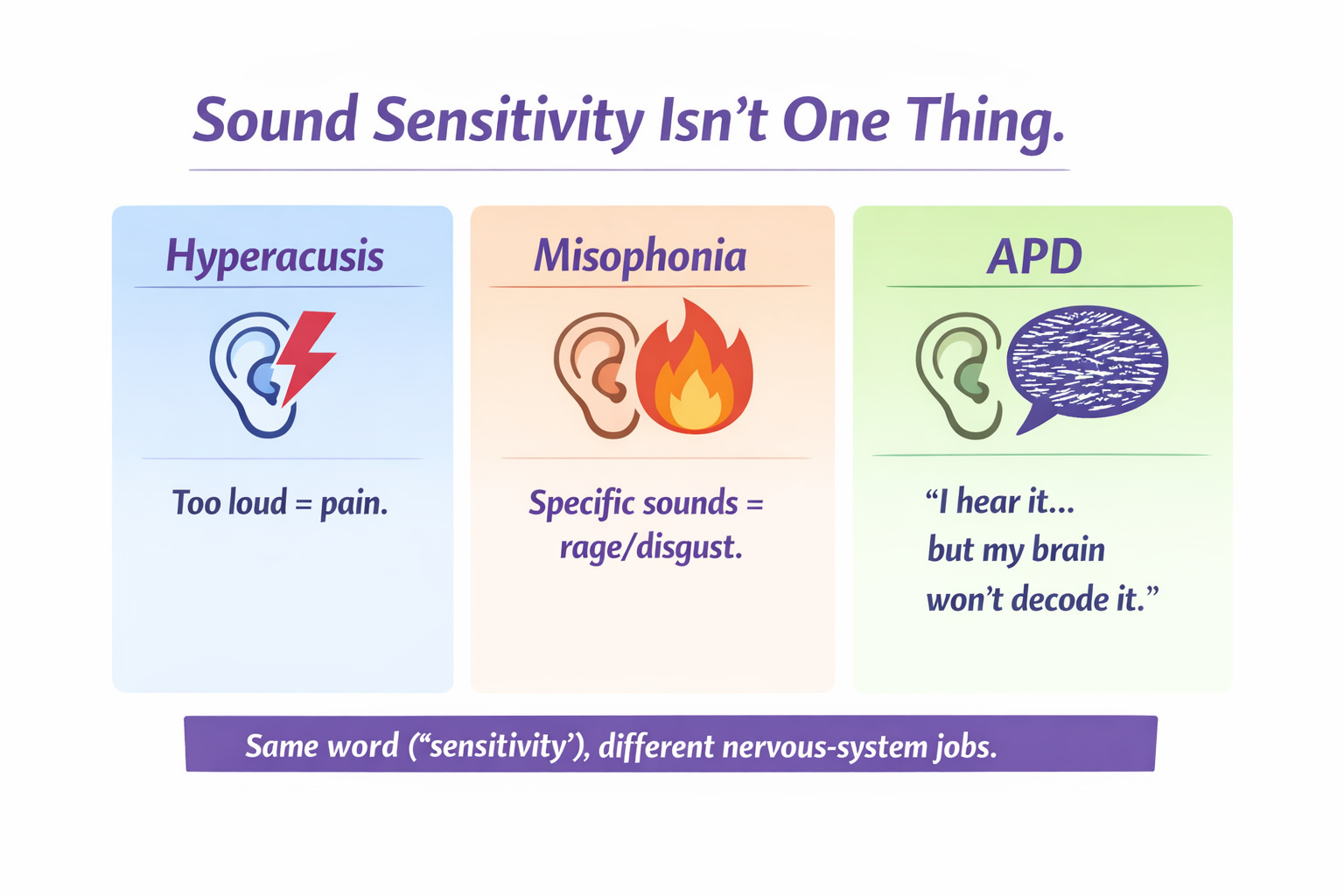
Research makes important distinctions between:
Hyperacusis = sound is physically too loud / painful (a loudness tolerance issue).
Misophonia = specific sounds trigger rage/disgust/panic (a threat/salience + emotion loop issue).
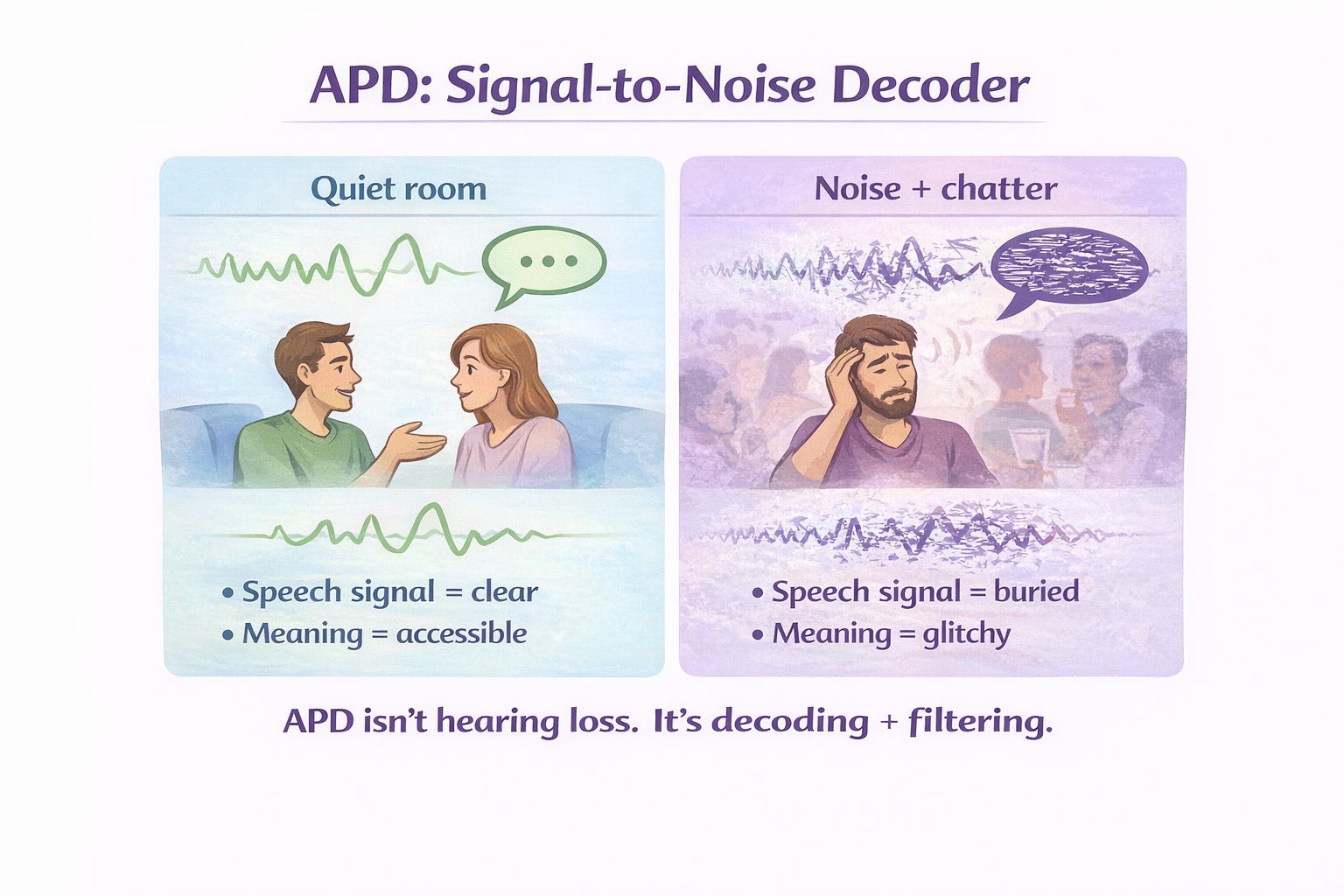
Auditory Processing Disorder (APD/CAPD) = your ears hear it, but your brain doesn’t decode it cleanly (a processing clarity issue—especially in noise).
If you’re AuDHD, you can have one, two, or the entire chaotic Pokémon evolution set at once—because autism and ADHD both skew sensory attention, filtering, and nervous-system reactivity in ways that can crank up auditory overwhelm. Recent work looking across autism-only, ADHD-only, and autistic+ADHD groups shows elevated auditory difficulties like distractibility and sound intolerance across neurodivergent profiles.
Let’s separate the sound profiles, map the neuroscience, and then get you strategies that actually match what’s happening.
The AuDHD “Sound System” in plain language
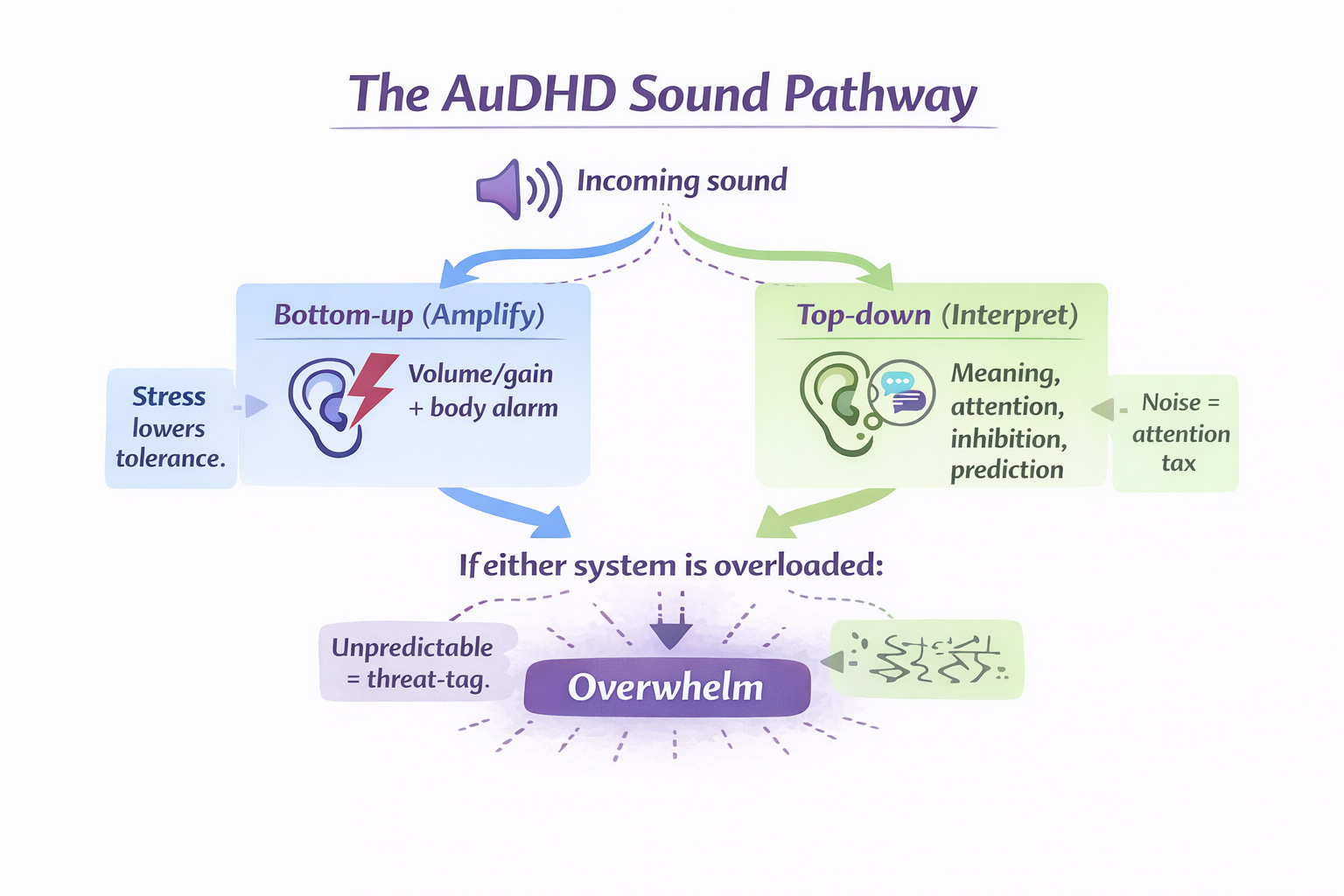
AuDHD brains often run two processes at the same time:
Amplification (bottom-up): incoming sound hits the system and your body reacts fast.
Interpretation (top-down): your brain tries to sort meaning, prioritize, and inhibit irrelevant input.
When either of those is off—too much gain, too much threat-tagging, too little clarity, too little filtering—sound stops being background… and becomes the whole room.
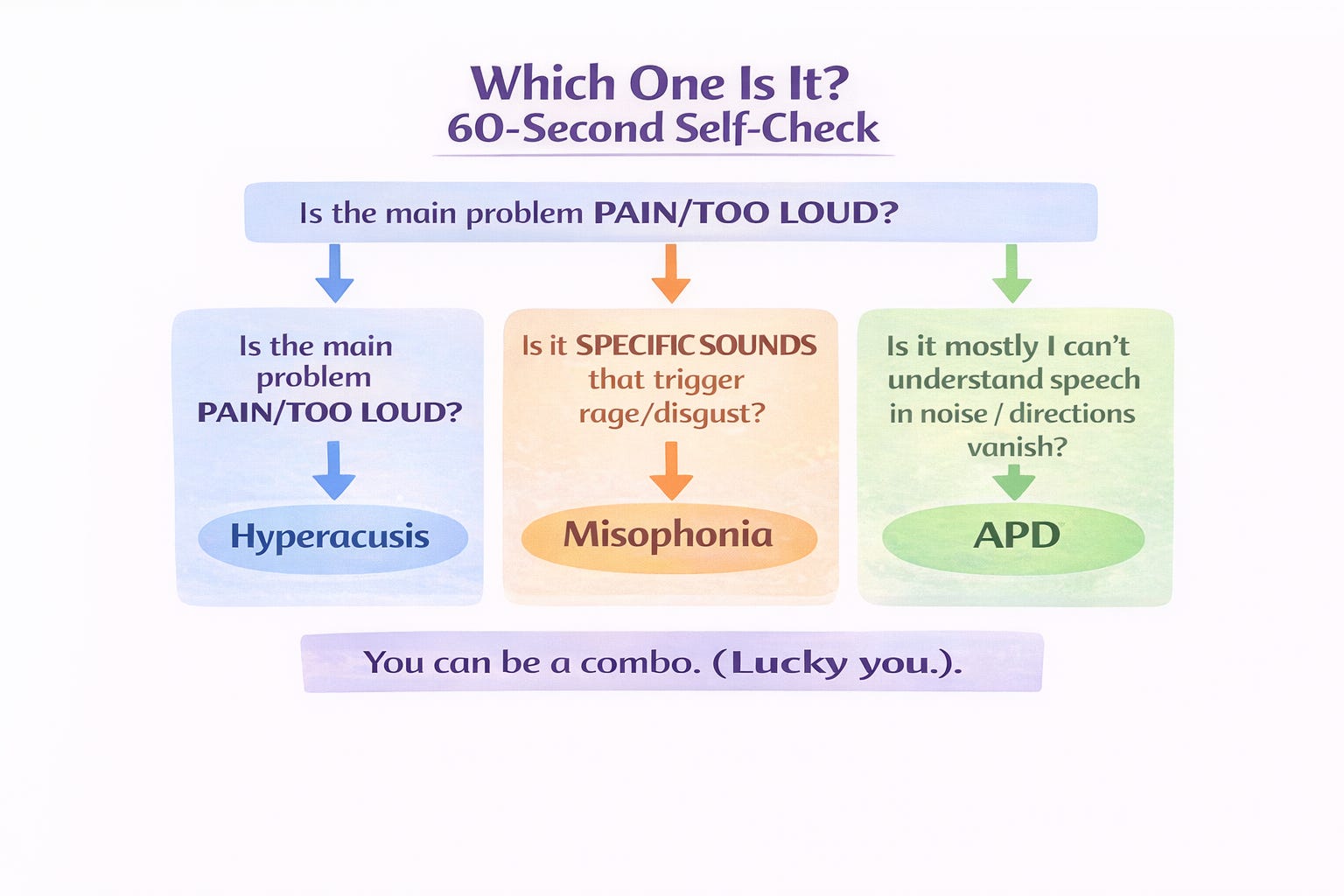
Quick “Which one is it?” mini-check
Hyperacusis (loudness pain / discomfort)
You’re not being dramatic: everyday sounds can feel too loud, even painful, because your loudness tolerance is reduced (often measured via loudness discomfort levels).
Key feature: it’s mainly about volume/intensity.
Misophonia (triggered rage/disgust)
This is not about loudness. It’s about pattern + meaning + social context (chewing, sniffing, pen clicking, breathing), and the reaction tends to be immediate anger/disgust + body arousal.
Key feature: it’s about specific trigger sounds, often human-generated.
APD / CAPD (auditory decoding + speech-in-noise struggle)
You can have normal hearing thresholds but still struggle to understand speech in noise, follow rapid speech, localize sound, or hold auditory directions in working memory.
Key feature: “I heard you… but I didn’t understand you.”
Profile 1: Hyperacusis — when loudness feels like injury
What it feels like
Sudden flinch, pain, pressure, or “my nerves are on fire” when sounds spike
You start pre-avoiding places: restaurants, gyms, classrooms, cinemas
You may feel exhausted after normal environments because you were bracing the whole time
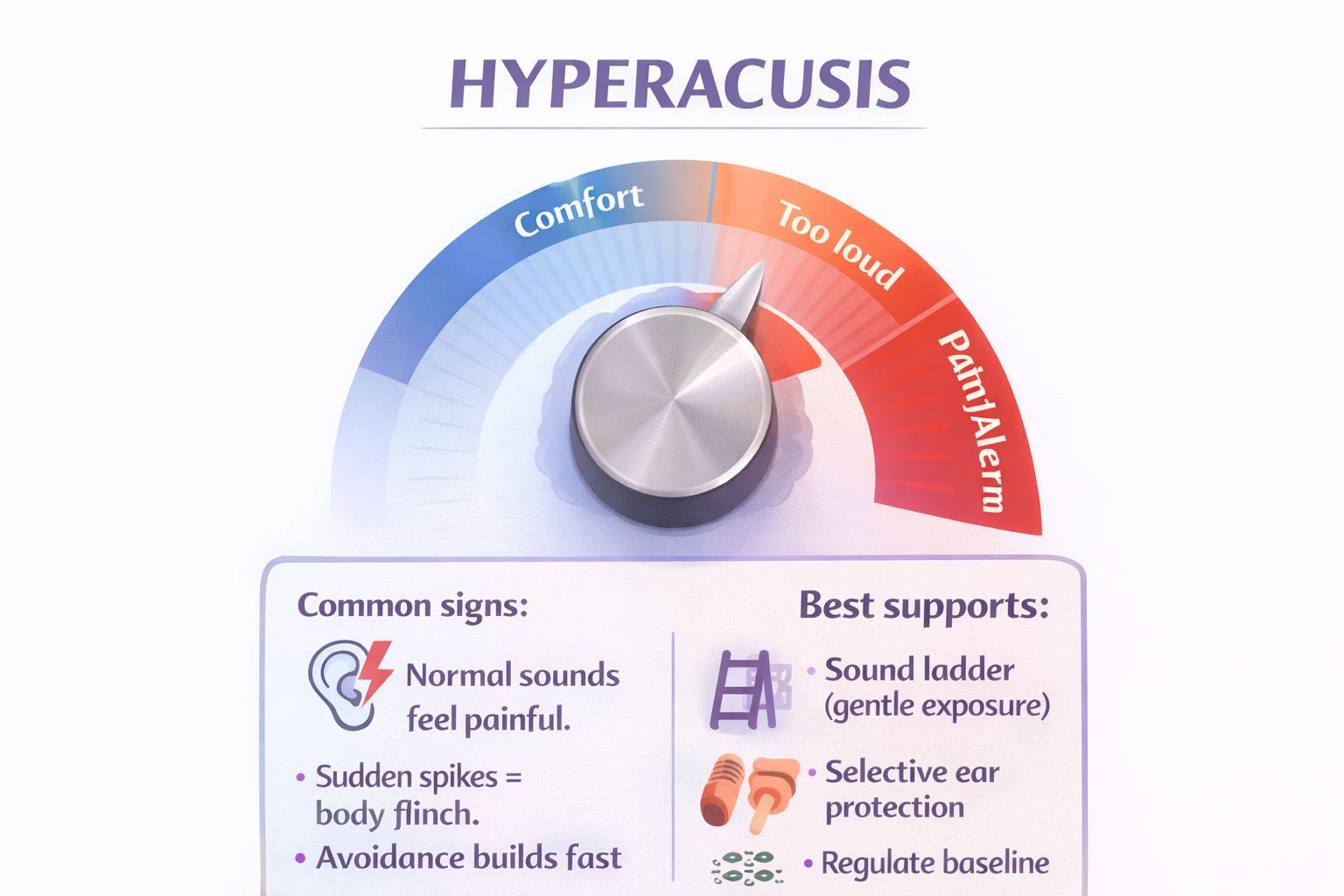
Hyperacusis is commonly described as decreased tolerance to sound, where normal levels are experienced as excessively loud or painful.
The neuroscience vibe: “the gain knob got turned up”
One major hypothesis is increased neural gain in the auditory system—basically, the brain’s volume amplifier is turned up, so moderate inputs get interpreted as too intense.
This can become a feedback loop:
sound → pain/discomfort → fear/avoidance → more vigilance → more sensitivity.
What helps (without accidentally making it worse)
1) Don’t overprotect 24/7
Wearing heavy hearing protection constantly can sometimes backfire by keeping your system in “fragile mode.” Many clinical discussions emphasize careful, structured approaches rather than pure avoidance.
Instead:
Use protection for true spikes (sirens, power tools, concerts)
Use softer tools for daily life (Loop-style filters, musician’s earplugs, lower attenuation)
2) Build “sound safety” gradually
Hyperacusis care often includes sound therapy / gradual sound enrichment approaches and addressing anxiety around sound.
Try:
Low-level background sound (fan, brown noise) for gentle desensitization
A “sound ladder” (start with tolerable sounds; move up slowly)
3) Reduce nervous system load, not just decibels
When your baseline stress is high, your tolerance plummets. Think: sleep debt + sensory chaos + deadlines = your auditory threshold drops.
Micro-regulators:
jaw unclench + long exhale
shoulder drop
2 minutes of walking pressure (wall push-ups count)
4) Rule out hearing-related contributors
Hyperacusis evaluation often involves audiology assessment and can co-occur with tinnitus or other conditions.
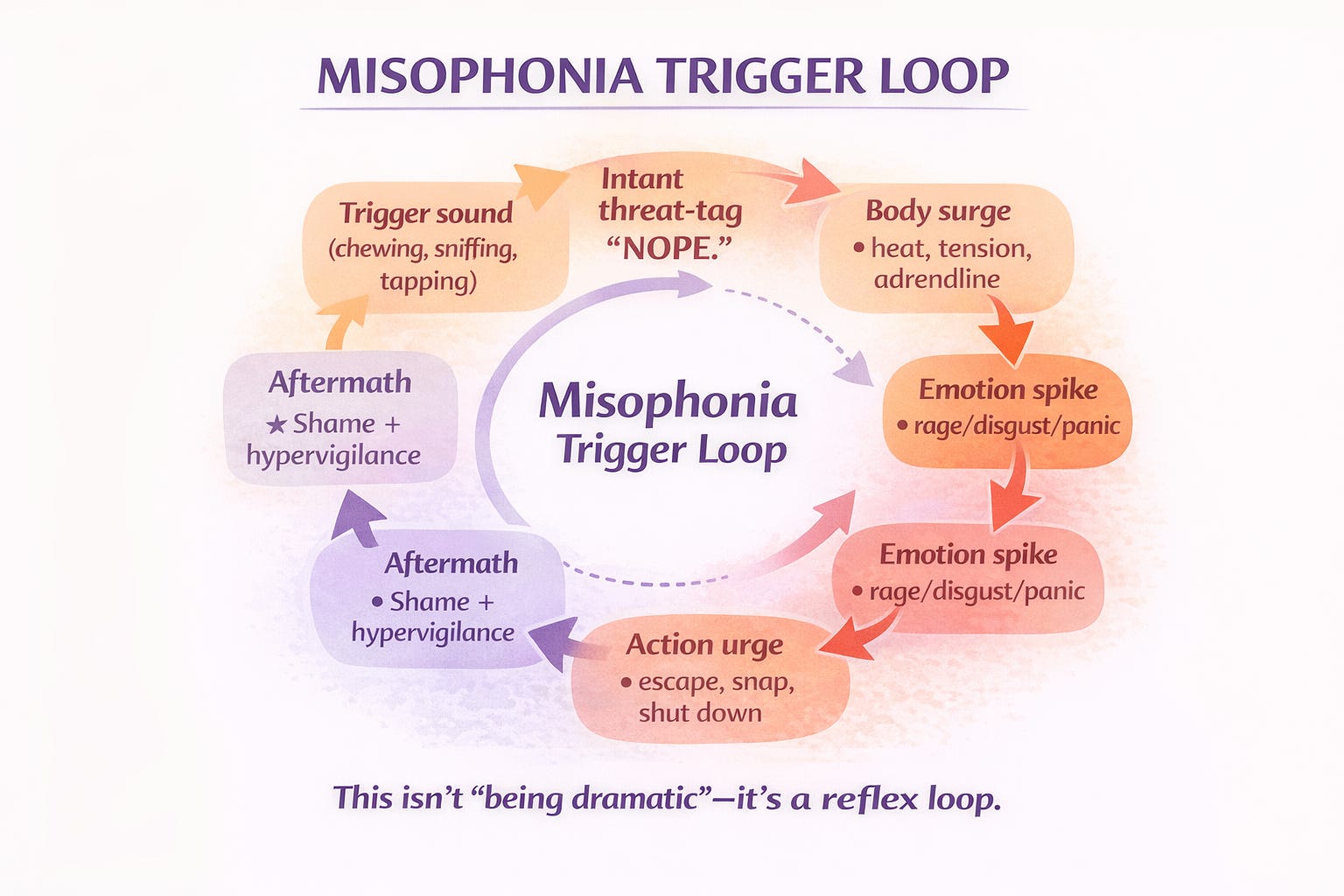
Profile 2: Misophonia — when a sound gets tagged as a threat
What it feels like
A specific sound hits and your body goes hot
The emotion is disproportionate (and you KNOW it) but it still floods you
You want to flee, shout, cry, or crawl out of your skin
Misophonia is widely described as intense negative emotional reactions (often anger/disgust) to specific trigger sounds, with significant distress and impairment.
The neuroscience vibe: salience network + “meaning alarm”
Neuroimaging work links misophonia to altered activity in regions involved in salience and emotion processing (including insula and anterior cingulate), along with strong physiological arousal.
Translation: your brain isn’t just hearing a sound—it’s stamping it with:
“This is disgusting / unsafe / intolerable — ACT NOW.”
For AuDHD folks, this often layers with:
inflexible attention shifting (sticky focus)
sensory gating differences
social stress (the fact it’s a person making the sound can intensify it)
What helps (that isn’t “just calm down”)
1) “Name the loop” without shaming yourself
Try this internal script:
“That’s the misophonia alarm.”
“This is a body surge, not a moral truth.”
“I can act without attacking.”
2) Pattern interrupts
Because triggers are fast, you need fast tools:
chew-gum yourself (give your auditory system competing input)
one earbud with neutral sound (brown noise / soft music)
“sound buffer object” (a scarf, hood, or pillow for subtle dampening)
3) Pre-negotiate, don’t white-knuckle
Misophonia-friendly agreements:
“If I tap your arm, can we pause chewing for 60 seconds?”
“Can we do crunchy foods at the table and soft foods on the couch?”
“I love you and my nervous system hates mouth sounds—both true.”
4) Exposure…but only the right kind
Some approaches explore gradual exposure paired with regulation, but misophonia is not simply “fear of loud sounds,” so generic desensitization can feel like torture if it’s not done thoughtfully.
5) Screen for overlap
A 2024 study in a clinical context noted misophonia can co-exist with hyperacusis and may show differing profiles.
Profile 3: Auditory Processing Disorder (APD/CAPD) — when clarity collapses
What it feels like
“I can hear you, but I can’t understand you” (especially with background noise)
Directions vanish unless they’re written
You mishear words, need repetition, or respond slowly
Phone calls are disproportionately hard
ASHA describes CAPD signs like difficulty understanding speech in noise or competing messages, longer response time, frequent requests for repetition, and difficulty following complex auditory directions.
APD is often described as difficulty listening/processing despite normal hearing thresholds.
The neuroscience vibe: decoding + timing + attention coordination
APD involves how the central auditory nervous system processes sound, not just whether your ears detect it.
And it can co-occur with attention and learning differences—including ADHD—because attention and auditory processing collaborate constantly.
In AuDHD life, APD often looks like:
auditory input gets blended (foreground and background feel the same “volume”)
working memory drops the sentence halfway through
your processing speed can’t keep up with rapid speech
What helps (immediately practical)
1) Change the channel: visual + written
You are not “bad at listening.” Your brain needs multimodal input.
Ask for bullet points in chat/email
Use captions (yes, even in-person—live caption apps exist)
Repeat back the key point: “So the plan is X by Friday, right?”
2) Improve signal-to-noise
sit with your back to the wall in restaurants
choose corners over center tables
request closed doors or quieter rooms
reduce reverb (rugs, curtains, soft surfaces—seriously, acoustics matter)
3) Auditory training / rehab approaches
Clinical discussions include auditory training and environmental supports as parts of management.
4) Stop doing “auditory-only” memory tasks
For AuDHD brains, verbal directions are basically disappearing ink. Externalize:
checklist
shared notes doc
voice-to-text dump + highlight action items
The overlap problem: why you might have a “combo platter”
You can absolutely have:
hyperacusis (pain with loudness) and
misophonia (rage at chewing) and
APD (speech-in-noise confusion)
And in AuDHD, the day-to-day presentation can change depending on:
stress level
sleep
hormonal shifts
environment acoustics
sensory “budget” already spent
This is why blanket advice like “try noise-canceling headphones” sometimes helps… and sometimes makes things worse (quieting everything can increase vigilance or reduce tolerance, depending on the profile).
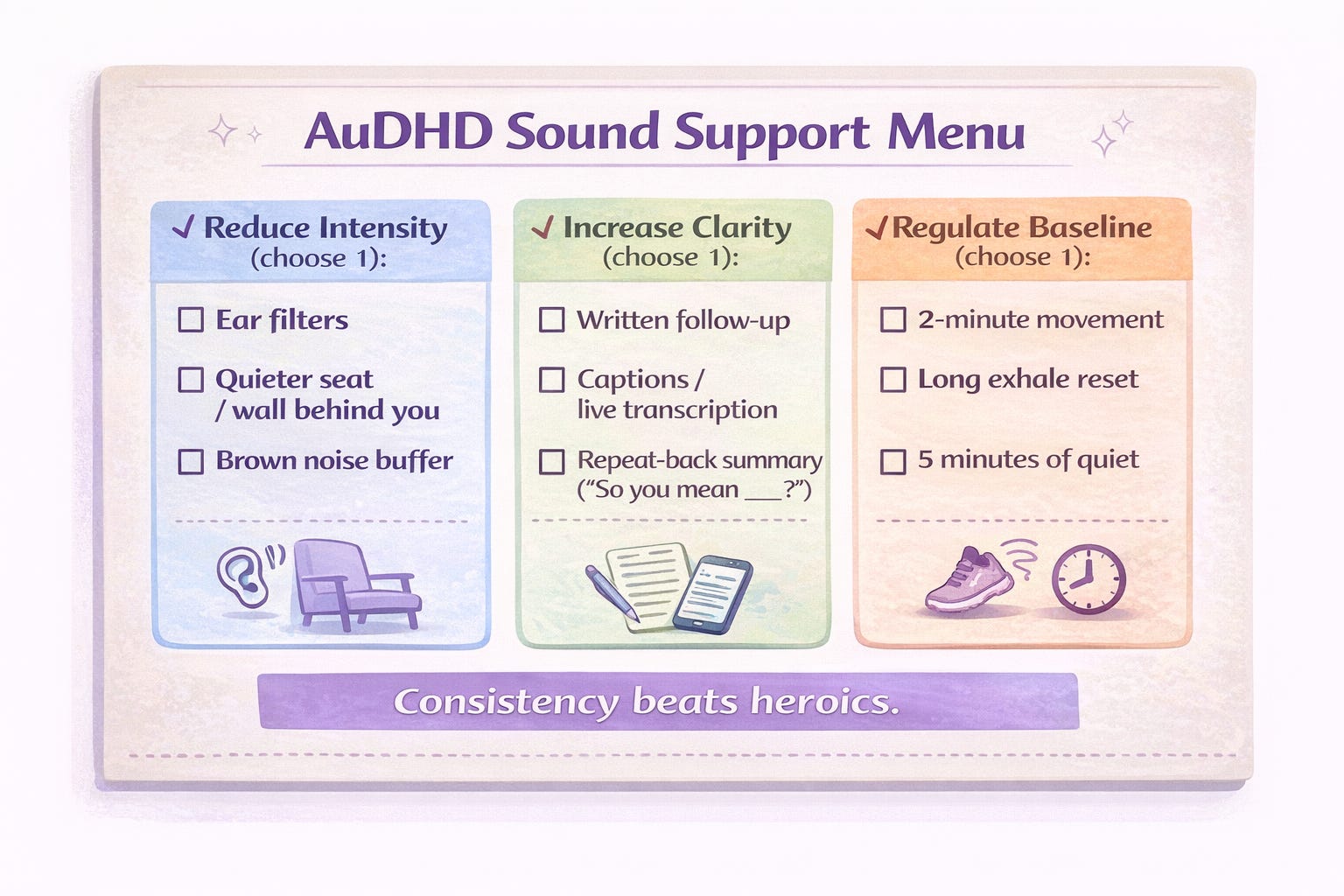
The AuDHD Sound Support Menu (mix-and-match)
Environment design
Create a quiet anchor zone (one room, one chair, one corner)
Add soft materials to reduce echo (rugs, throws, curtains)
Keep a “sound kit” by the door: ear filters, earbuds, gum, sunglasses (light + sound gang up)
Communication scripts (steal these)
“I process best with written follow-up—can you text me the main points?”
“If you’re talking while there’s background noise, I’ll miss pieces. Can we move?”
“I need 10 seconds to decode what you said—pause with me.”
Recovery rituals (because your brain needs cooldown)
5 minutes of silence after noisy transitions
warm shower or deep pressure
“auditory palate cleanser”: soft music, nature sounds, or steady brown noise
Professional supports to consider
Audiologist for hyperacusis/APD evaluation and guidance
ENT if there are medical contributors
Therapy support for coping, distress tolerance, and reducing the shame spiral (especially for misophonia)
(Not medical advice—just a “here are the lanes” map.)
Reflection journal prompts
(because patterns = power)
Identify your profile
When sound overwhelms me, is it more like pain, rage/disgust, or confusion?
What are my top 5 worst sounds—and what do they have in common (volume, pattern, human-made, unpredictability)?
Do I struggle more with noise level or speech clarity?
Track your nervous system
On days my sound tolerance is low, what else is true? (sleep, hunger, stress, social load)
What does my body do first—jaw clench, shoulders up, stomach drop, heat, tears?
Build your “sound boundaries”
What’s one sound boundary I can set without apologizing?
What accommodations help me most at home? At work? In public?
Rewrite the story
If my brain had subtitles, what would it say during a trigger moment?
What would I tell a friend who had my exact sound profile?
Plan experiments (tiny and measurable)
This week, I will test one change: _______. I’ll rate my overwhelm before/after (0–10).
If you want the fastest “do this tomorrow” plan
Pick one from each column:
Reduce intensity: ear filters OR quieter seat OR sound buffer (brown noise)
Increase clarity: written follow-up OR captions OR repeat-back summary
Regulate baseline: 2-min movement OR long exhale practice OR 5-min quiet reset
Consistency beats heroics. Your ears aren’t the villain—your system is just overclocked.
I hit the jackpot and have all three! I think the hardest part for me is the misophonia because the reaction is so strong and instantaneous and it is triggered by people I love who are just chewing, and it takes all my willpower not to snap angrily at them (and often, that fails). So thank you for this post!